|
|
|
|
Retroperitoneal sarcomas (RPS) are rare malignant tumours (0.5 to 1% of malignant tumours) [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref],2]Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20
The retroperitoneal location accounts for 12% to 15% of soft tissue [ 3Toulmonde M., Bonvalot S., Méeus P., Stoeckle E., Riou O., Isambert N., et al. Retroperitoneal sarcomas: patterns of care at diagnosis, prognostic factors and focus on main histological subtypes: a multicenter analysis of the French Sarcoma Group. Ann Oncol 2014 ; 25 (3) : 735-742 [cross-ref]] sarcomas and some histological types are more represented [ 1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref]].
The vast majority of RPSs are sporadic. However 2 risk factors have been identified [2Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20]:
|
• |
Radiotherapy, which causes radiation-induced sarcomas (mainly malignant fibrous histiocytomas, extra-skeletal osteosarcomas and fibrosarcomas) characterised by their aggressiveness and poor prognosis. |
|
• |
Several hereditary diseases such as neurofibromatosis type I (associated with malignant schwannoma), RB gene alterations or Li Fraumeni syndrome (alteration of the tumour suppressor gene TP53). |
RPS grows by successive centrifugal spurts which delimit a pseudo-tumour capsule, always invaded and sometimes crossed by tumour buds which contaminate the adjacent retroperitoneal space [2Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20]. Any breach in the pseudo-capsule (lumpectomy or surgical biopsy) causes tumour dissemination.
|
|
|
Clinical diagnosis (Figure 1)
|
|
|
|
|
|
Revealing clinical circumstances
|
RPS has a large tumour volume at the time of diagnosis due to the space available in the RP (18 cm in the greatest median dimension [4Cates J.MM. Performance Analysis of the American Joint Committee on Cancer 8th Edition Staging System for Retroperitoneal Sarcoma and Development of a New Staging Algorithm for Sarcoma-Specific Survival. Ann Surg Oncol 2017 ; 24 (13) : 3880-3887 [cross-ref]]).
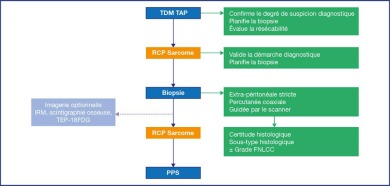
Figure 1.
Diagnostic approach for RPS.
Apart from incidental diagnoses on non-dedicated imaging, pain (lumbar, abdominal), and ureteral or small intestine compressions are the main diagnostic features. RPS should be suspected when such tumours are discovered until the contrary is proven by the histological assessment.
Distant metastasis is rare on initial diagnosis but is always a possibility, especially in the event of a relapse or a high-grade leiomyosarcoma.
|
| Thoraco-abdomino-pelvic scan (TAP CT) |
The TAP CT scan with injection of a contrast agent is essential for the diagnostic process and the development of the therapeutic plan [5]:
|
• |
Consider a positive diagnosis: with a lesion located at the retroperitoneum, not developed to the detriment of an organ. The retroperitoneal character is sometimes difficult to assess when masses are large, but displacement of the retroperitoneal organs is a useful sign. The tumour can pass through anatomical openings, which is characteristic of the method of development. RPS typically has no nourishing artery. |
|
• |
In certain cases, consider the histological characteristic: liposarcomas may have a fat density component and vascularized septa. The disappearance of the inferior vena cava is a sign of sarcoma of the vena cava (leiomyosarcoma, angiosarcoma). |
|
• |
Plan the biopsy procedure for the primary tumour or metastasis. |
|
• |
Perform lymph node and systemic staging (up to 50% pulmonary metastases on diagnosis of leiomyosarcoma). |
|
• |
Examine the resectability criteria. |
Abdominal MRI is indicated in patients who are allergic to iodinated contrast media, as a complement to a CT scan without injection, or in cases where a CT scan is difficult to perform. This can provide an improvement in the specification of muscular, bone, foraminal or vascular metastasis. In the pelvis, MRI can be useful to delineate the lesion.
The MRI protocol includes classical T1 and T2, fat saturation, diffusion and dynamic sequences after Gadolinium injection. The boundaries of the tumour can be examined in all planes by virtue of the body coil.
Radiotherapy can help to delineate the volume for treatment and include peritumoral oedema for optimal results [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]].
Ultrasound does not rule out the diagnosis, but it can lead to the initial discovery of a mass that initiates the diagnostic process.
18FDG PET is not indicated in the initial diagnosis due to the variability in histological types and grades encountered. It is not discriminating enough to distinguish low-grade sarcomas from benign tumours [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]]. Nevertheless, It can play a role in the follow-up of tumour progression in recurrence, given the sensitivity and specificity which are superior to those of CT scan in this context [6Roberge D., Vakilian S., Alabed Y.Z., Turcotte R.E., Freeman C.R., Hickeson M. FDG PET/CT in Initial Staging of Adult Soft-Tissue Sarcoma. Sarcoma 2012 ; 2012 : 960194], or in the evaluation of aggressive forms.
Bone scintigraphy may be of interest in the differential diagnosis of primary bone tumour with adjacent soft tissue involvement.
In cases where excision involves one of the kidneys, a biological evaluation and DMSA scan of renal function are recommended [7Casali P.G., Abecassis N., Bauer S., Biagini R., Bielack S., Bonvalot S., et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 28 mai 2018 ; 29 : iv51-67], in preparation of possible nephrological management.
|
|
|
Diagnostic approach (Figure 1)
|
|
|
When RPS is suspected, and before the biopsy is performed, the case should be discussed in a specialised MTM. The French sarcoma reference network (RRePS-TMV) can be solicited. They have 3 coordinating centres and 19 reference centres (www.infosarcomes.org) throughout France.
Through this approach, the suspicion can be confirmed, the biopsy optimised (yield and safety against dissemination), and the therapeutic strategy, necessarily multidisciplinary, often multimodal and, in all cases, highly specialised, can be planned and prepared.
Although it is revealed on imaging, a positive diagnosis is histological, through biopsy. It enables the formulation of several differential diagnoses, including benign tumours, extragonadal germ cell tumours and lymphomas [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref],8Van Houdt W.J., Schrijver A.M., Cohen-Hallaleh R.B., Memos N., Fotiadis N., Smith M.J., et al. Needle tract seeding following core biopsies in retroperitoneal sarcoma. Eur J Surg Oncol 2017 ; 43 (9) : 1740-1745 [cross-ref]]. RPSs account for only one-third of the retroperitoneal tumours [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]]
Radiologically-guided percutaneous biopsy is performed by extraperitoneal approach along a short path, using a sheathed guidewire (coaxial needle) [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref],8Van Houdt W.J., Schrijver A.M., Cohen-Hallaleh R.B., Memos N., Fotiadis N., Smith M.J., et al. Needle tract seeding following core biopsies in retroperitoneal sarcoma. Eur J Surg Oncol 2017 ; 43 (9) : 1740-1745 [cross-ref]]. It is currently the standard for sampling [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
CT guidance helps to identify the path and an area of interest in the tissue (excluding necrotic and cystic areas, preferably in the least adipose portion) [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]]. Where technically and reasonably possible, sampling should include different areas. The diameter of the needle is chosen by the radiologist according to the path and the risk of haemorrhage. An 18G needle or better yet, a 16G, is usually suitable for histological diagnosis. The risk of path contamination is low, although it does exist and does not appear to be associated with more local recurrences [8Van Houdt W.J., Schrijver A.M., Cohen-Hallaleh R.B., Memos N., Fotiadis N., Smith M.J., et al. Needle tract seeding following core biopsies in retroperitoneal sarcoma. Eur J Surg Oncol 2017 ; 43 (9) : 1740-1745 [cross-ref]]. The path can be tattooed for later identification to enable the excision [7Casali P.G., Abecassis N., Bauer S., Biagini R., Bielack S., Bonvalot S., et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 28 mai 2018 ; 29 : iv51-67]. When the diagnosis is not the one that was anticipated, the biopsy path could be affected by the surgical excision.
It was recommended that a fresh sample be sent to the pathological laboratory for possible freezing based on the quantity of biopsy material to enable subsequent molecular testing [7Casali P.G., Abecassis N., Bauer S., Biagini R., Bielack S., Bonvalot S., et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 28 mai 2018 ; 29 : iv51-67]. Molecular studies can now be performed on formalin-fixed paraffin-embedded tissue.
Surgical biopsy may provide more material but the indication should be balanced by the risk of seeding resulting from pseudocapsule rupture. The decision should be made by the reference centre [7Casali P.G., Abecassis N., Bauer S., Biagini R., Bielack S., Bonvalot S., et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 28 mai 2018 ; 29 : iv51-67]. It should be strictly extraperitoneal. During definitive treatment, resecting the surgical route is required. The transsphincteric and transvaginal approaches are forbidden considering the affinity of recurrences for scars which worsens the functional prognosis in these contexts.
Regardless of the sampling method, the transperitoneal approach should be the last resort for diagnosis, after discussion of the case in a specialised multidisciplinary meeting [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]].
The definitive histological analysis is performed by a specialised pathologist [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
RPS is classified according to the resemblance to the original mesenchymal tissue.
Liposarcoma is the most common histological form (30 to 60% of the cases) [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref],11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. It is a locally aggressive tumour composed of adipose tissue. Liposarcoma is subdivided into well-differentiated (45.8% of cases), dedifferentiated (44.8%), myxoid (4.7%) and pleomorphic (0.8%) forms [11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Undifferentiated forms confer a non-adipocyte component of high grade. In doubtful cases, the histological diagnosis is supported by an amplification of the MDM2 gene by fluorescent in situ hybridisation (FISH) or colorimetric in situ hybridisation (CISH). Since (benign) lipomas are extremely rare in the retroperitoneum, the diagnosis should not be made without this assessment. In contrast, the dedifferentiated form is very common in the retroperitoneum and can also be found in the spermatic cord [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref]].
Leiomyosarcoma (20 to 30% of the cases) [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref],11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]] includes smooth muscle differentiation cells. Retroperitoneal and pelvic locations are the most common. A mass developed to the detriment of a retroperitoneum vessel (inferior vena cava, aorta, gonadal vessels in particular) is suggestive of this type of tumour [11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Leiomyosarcomas are among the most biologically aggressive sarcomas and are associated with a high rate of mortality [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref]]. Their metastatic spread is mainly haematogenous [12Gronchi A., Strauss D.C., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann Surg 2016 ; 263 (5) : 1002-1009 [cross-ref]].
Malignant fibrous histiocytoma account for less than 10% of the cases [11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Most diagnoses of MFH have been found to belong to another undifferentiated histological subtype, often liposarcoma. In practice, this term should no longer be used.
Other sarcomas are rarer [11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]: fibrosarcoma, rhabdomyosarcoma, synovial sarcoma, Ewing's sarcoma or malignant schwannoma.
The main prognostic criteria are size, histological type and grade according to the criteria defined by the French federation for cancer control (FNCLCC).
Leiomyosarcomas and angiosarcomas are aggressive tumours for which histological grade is not a discriminating criterion. In addition, regardless of the histological subtype, the criteria taken into account to define the FNCLCC grade are the mitotic index, cell differentiation and tumour necrosis.
The sum of each of the criteria produces a score ranging from 2 to 8, translated into 3 grades (Table 1) [13Trojani M., Contesso G., Coindre J.M., Rouesse J., Bui N.B., de Mascarel A., et al. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int J Cancer 1984 ; 33 (1) : 37-42 [cross-ref]].
The TNM classification of retroperitoneal sarcomas is primarily determined by tumour size [14Amin M.B., Edge S., Greene F., Byrd D.R., Brookland R.K., Washington M.K., et al. AJCC Cancer Staging Manual New York: Springer (2017). ] (Table 2). This classification has been criticised, particularly with regard to stage T, because the median size at diagnosis classifies the majority of RPSs as stage T4, despite a larger sub-division of sizes in the latest update [15Pasquali S., Gronchi A. Neoadjuvant chemotherapy in soft tissue sarcomas: latest evidence and clinical implications. Ther Adv Med Oncol 2017 ; 9 (6) : 415-429 [cross-ref]]. As a continuous variable, tumour size has a modest effect on survival (HR 1.004; p=0.04) in contrast to the T4 stage (HR 1.3; p < 0.001 ) which remains a less powerful prognostic factor than a high grade (HR 2,5; p < 0.001 ) or macroscopically incomplete resection R2 (HR 1.97; p < 0.001) [16Fisher S.B., Chiang Y-J, Feig B.W., Cormier J.N., Hunt K.K., Torres K.E., et al. An Evaluation of the Eighth Edition of the American Joint Committee on Cancer (AJCC) Staging System for Retroperitoneal Sarcomas Using the National Cancer Data Base (NCDB): Does Size Matter?. Am J Clin Oncol 2019 ; 42 (2) : 160-165 [cross-ref]].
The AJCC stages are defined by a synthesis of the TNM stage and the FNCLCC grade [14Amin M.B., Edge S., Greene F., Byrd D.R., Brookland R.K., Washington M.K., et al. AJCC Cancer Staging Manual New York: Springer (2017). ] (Table 3). This simple staging could be inadequate and the prognosis assessment could be more discriminating by taking into account: tumour size, histological type (favourable/unfavourable) and FNCLCC grade [4Cates J.MM. Performance Analysis of the American Joint Committee on Cancer 8th Edition Staging System for Retroperitoneal Sarcoma and Development of a New Staging Algorithm for Sarcoma-Specific Survival. Ann Surg Oncol 2017 ; 24 (13) : 3880-3887 [cross-ref]]. Multiple nomograms have been developed, including some specific to retroperitoneal sarcoma [17Callegaro D., Miceli R., Gladdy R.A. Prognostic models for RPS patients-Attempting to predict patient outcomes. J Surg Oncol 2018 ; 117 (1) : 69-78 [cross-ref]].
|
|
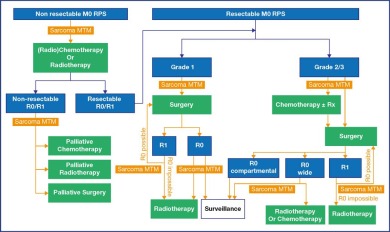
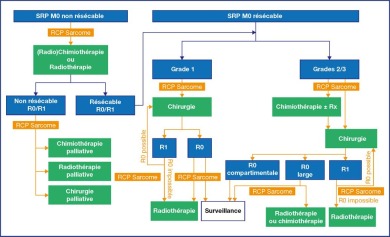
As the cornerstone of curative treatment, surgical excision of RPS meets oncological requirements for quality of excision and technical requirements for resectability. Macroscopically complete resection improves survival although the local recurrence rate remains high overall [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]]. Under these conditions, with a significant median tumour volume and common combined procedures, discussion of the approach is currently restricted, since the rare laparoscopic studies are biased by a limited volume of excisions and insufficient follow-up [18Gronchi A., Crago A., Raut C.P. Minimally Invasive Surgery for Retroperitoneal Sarcoma: Just Because We Can Does Not Mean We Should. Ann Surg Oncol 2018 ; 25 (8) : 2129-2131 [cross-ref]].
Figure 2.
Therapeutic approach to localised RPS.
The oncological objective is tumour resection en bloc at the healthy microscopic margin (R0), especially since there is no systemic salvage treatment for macroscopically incomplete surgery and since tumour invasion promotes peritoneal dissemination (Sarcomatosis). The pseudocapsule surrounding the sarcoma consists of a surface of densified tumour cells which is not a suitable cleavage plane.
The notion of compartmental surgery is derived from the principles concerning sarcomas of the extremity for which a margin of healthy muscle surrounding the tumour is systematically removed [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
It consists of the excision of an abdominal quadrant which holds at least the organs that are pushed back and sometimes the organs in contact [19Bonvalot S., Raut C.P., Pollock R.E., Rutkowski P., Strauss D.C., Hayes A.J., et al. Technical considerations in surgery for retroperitoneal sarcomas: position paper from E-Surge, a master class in sarcoma surgery, and EORTC-STBSG. Ann Surg Oncol 2012 ; 19 (9) : 2981-2991 [cross-ref]]. This is especially true for the small intestine and the upper urinary tract. An orthopaedic procedure may be necessary for the very wide exposure required for this en bloc compartmental resection (spine, sacrum).
A retrospective study of compartmental resections reported histological invasion of 65% of the organs suspected to be invaded, 26% of adherent organs, 19% of enveloped organs but none of the other organs involved in en bloc resection [20Fairweather M., Wang J., Jo V.Y., Baldini E.H., Bertagnolli M.M., Raut C.P. Surgical Management of Primary Retroperitoneal Sarcomas: Rationale for Selective Organ Resection. Ann Surg Oncol 2018 ; 25 (1) : 98-106 [cross-ref]].
Although the objective of this surgery is macroscopically healthy margins, it is associated with a higher level of morbidity, especially when the duodenum, large vessels, pancreas or major nerves are involved [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
It is a difficult, technically complex surgery that should be performed by a multidisciplinary team. Morbidity is high, including in reference centres, with 16.4% Clavien-Dindo ⥠3 complications (particularly in the case of major vascular resection or pancreatic surgery) and 1.8% deaths at 30 days [21MacNeill A.J., Gronchi A., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Postoperative Morbidity After Radical Resection of Primary Retroperitoneal Sarcoma: A Report From the Transatlantic RPS Working Group. Ann Surg 2018 ; 267 (5) : 959-964 [cross-ref]].
A dedicated multidisciplinary team seems essential to develop the therapeutic plan and ensure its implementation with the lowest level of morbidity [22Maurice M.J., Yih J.M., Ammori J.B., Abouassaly R. Predictors of surgical quality for retroperitoneal sarcoma: Volume matters. J Surg Oncol 2017 ; 116 (6) : 766-774 [cross-ref]].
In the absence of randomised studies that evaluate the benefits of wide resections, some have suggested a strategy based on anatomical and histological data [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]], the patients who could benefit most from this surgery being those with an aggressive subtype such as high-grade undifferentiated liposarcoma [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]]. In other histologies [23Ikoma N., Roland C.L., Torres K.E., Chiang Y.J., Wang W.L., Somaiah N., et al. Concomitant organ resection does not improve outcomes in primary retroperitoneal well-differentiated liposarcoma: A retrospective cohort study at a major sarcoma center. J Surg Oncol 2018 ; 117 (6) : 1188-1194 [cross-ref]], a wide R0 resection may be sufficient, corresponding to a healthy margin resection with a healthy tissue border and no systematic organ sacrifice.
In France, a retrospective study noted an R0 resection rate of 41.9% in the NetSarc network centres (median volume from 2010 to 2017: 23 cases [3-209]) compared to 12.3% in non-network centres (median volume: 1 case [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref], 2Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20]) [24Bonvalot S., Gaignard E., Stoeckle E., Meeus P., Decanter G., Carrere S., et al. Survival Benefit of the Surgical Management of Retroperitoneal Sarcoma in a Reference Center: A Nationwide Study of the French Sarcoma Group from the NetSarc Database. Ann Surg Oncol 2019 ; 26 (7) : 2286-2293 [cross-ref]].
The technical possibilities for surgical excision or resectability of the tumour heavily influence the therapeutic strategy. The expertise of a reference centre is particularly required in order to assess the perioperative vital risk and the extent of functional harm (length of small intestines, genitourinary tract).
The tumour resectability rate is now up to 80%. The main criterion for tumour non-resectability is circular encapsulation of the superior mesenteric artery. Conversely, in traspinal invasion by an intervertebral foramen, invasion or circumferential extension to the aorta, invasion of the vena cava, and a pan-abdominal character require technical adaptations that enable resection under acceptable conditions.
Local recurrence occurs in 22 to 84% of the cases depending on the histological subtype, grade and quality of the initial resection [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
While 85% of the RPSs resected with a curative intent may result in a macroscopically complete resection (R0/R1) in the first surgery, this rate is less than 50% in second-line surgery [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
R0 resection of recurrent RPS can be interpreted as the only curative option but the limited chances of progression-free survival should be identified in the MTM to weigh the indication for wide resection with organ sacrifice/function [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540]. Morbidity/mortality is important, so assessment of the patient's general health status is an important selection [10] criterion to avoid impairment of quality of life when recovery is not ensured [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
The probability of complete resection reduces with the number of recurrences [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]] and the notion of fragmentation in the field of the initial tumour. The prognosis worsens with the number of nodules of peritoneal carcinomatosis [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
Neoadjuvant therapy may be indicated particularly in case of leiomyosarcoma, dedifferentiated liposarcoma, pleomorphic sarcoma, solitary fibrous tumours and synovial sarcoma [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
Visceral metastases are present in 10 - 20% of the cases at diagnosis and rarely constitute the site of first recurrence of the disease [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]]. Metastasectomy may have a survival benefit in selected oligometastatic patients [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540]. Surgical excision of any number of lung metastases has shown a survival benefit [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]], which is not the case for liver metastases where surgery is not the standard [19Bonvalot S., Raut C.P., Pollock R.E., Rutkowski P., Strauss D.C., Hayes A.J., et al. Technical considerations in surgery for retroperitoneal sarcomas: position paper from E-Surge, a master class in sarcoma surgery, and EORTC-STBSG. Ann Surg Oncol 2012 ; 19 (9) : 2981-2991 [cross-ref]].
In the presence of synchronous abdominal and distant recurrence, systemic treatment should be considered at first within a multimodal approach [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref], 10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
The value of adding radiotherapy is supported by a low level of evidence and is essentially based on the extrapolation of the results obtained for local control of high-grade sarcomas of the extremities, sometimes using older irradiation technologies [26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. Retroperitoneal location and the proximity of radiosensitive structures complicate irradiation modalities.
The timing of radiation therapy is controversial:
|
• |
Neoadjuvant radiotherapy is based on the theoretical optimisation of tissue oxygenation before surgery, easier contouring, the advantage of the tumour pushing back the radiosensitive organs, and a lower dose level than in the adjuvant context. The recommended dose is 50-50.4 Gy in fractions of 1.8-2 Gy and boosts can be added on areas at risk for positive margins [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. Surgery is offered 4 to 8 weeks after the end of radiotherapy. Retrospective studies support this modality with respect to overall survival but do not provide all the expected details, in particular those concerning recurrence and toxicity [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. A recent meta-analysis identified a benefit in progression-free and overall survival of perioperative radiotherapy compared to surgery alone, which is more marked in neoadjuvant therapy [ 27Diamantis A., Baloyiannis I., Magouliotis D.E., Tolia M., Symeonidis D., Bompou E., et al. Perioperative radiotherapy versus surgery alone for retroperitoneal sarcomas: a systematic review and meta-analysis. Radiol Oncol 2020 ; 54 (1) : 14-21 [cross-ref]]. A retrospective TARPSWG study did not confirm this benefit after statistical adjustment [ 28Haas R.LM., Bonvalot S., Miceli R., Strauss D.C., Swallow C.J., Hohenberger P., et al. Radiotherapy for retroperitoneal liposarcoma: A report from the Transatlantic Retroperitoneal Sarcoma Working Group. Cancer 2019 ; 125 (8) : 1290-1300 [cross-ref]]. The prospective randomised trial EORTC STRASS (NCT01344018), which completed inclusion in 2018, randomised patients with non-metastatic RPS between surgery alone and neoadjuvant radiotherapy followed by surgery. The main objective was intra-abdominal relapse-free survival. The results, which are still pending, will be decisive in future indications for radiotherapy.
|
|
• |
Postoperative adjuvant radiotherapy concerns all or part of the operating field, which can be identified by surgical clips. The overall survival data from the SEER database are contradictory [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref], 29Bates J.E., Dhakal S., Mazloom A., Constine L.S. The Benefit of Adjuvant Radiotherapy in High-grade Nonmetastatic Retroperitoneal Soft Tissue Sarcoma: A SEER Analysis. Am J Clin Oncol 2018 ; 41 (3) : 274-279]. The main limitation is late morbidity, reported between 5 and 40% of the cases for doses of 50 to 60 Gy [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. The use of « spacers » (in particular breast implants, to move the intestinal loops away from the area to be irradiated) has been reported, not without associated morbidity [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. The practice of extensive primary surgery and neoadjuvant radiotherapy have drastically reduced the indications for treatment [ 30Almond L.M., Gronchi A., Strauss D., Jafri M., Ford S., Desai A. Neoadjuvant and adjuvant strategies in retroperitoneal sarcoma. Eur J Surg Oncol 2018 ; 44 (5) : 571-579 [cross-ref]].
|
|
• |
The results of brachytherapy and intraoperative radiotherapy were mixed and associated with significant morbidity [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. Moreover, due to the rate of digestive complications, brachytherapy in the upper abdomen should be abandoned [ 31Naghavi A.O., Fernandez D.C., Mesko N., Juloori A., Martinez A., Scott J.G., et al. American Brachytherapy Society consensus statement for soft tissue sarcoma brachytherapy. Brachytherapy 2017 ; 16 (3) : 466-489 [cross-ref]].
|
|
• |
Emerging therapies (protons, carbon ions) are being developed to improve the efficacy and reduce the radiotoxicity of these adjuvant modalities [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]].
|
All in all, radiotherapy in multimodal treatment associated with surgery would appear to improve local control according to certain modalities (rather preoperative) and for certain tumours (well circumscribed, high grade), the identification of which requires improvement by inclusion in prospective trials.
The rationale for the use of perioperative chemotherapy in RPS is based on concepts such as preoperative cytoreduction, micro-metastatic sterilisation, and the evaluation of chemosensitivity on resection specimens:
|
• |
In a neoadjuvant context, chemotherapy allows objective responses (with the exception of well-differentiated non-chemosensitive liposarcoma) of approximately 21-33% [ 11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]], particularly in terms of tumour volume. It is discussed for large, high-grade tumours, especially when an associated nephrectomy is planned [ 15Pasquali S., Gronchi A. Neoadjuvant chemotherapy in soft tissue sarcomas: latest evidence and clinical implications. Ther Adv Med Oncol 2017 ; 9 (6) : 415-429 [cross-ref]], but the low response rate should not delay complete resection for a resectable mass. Traditionally, molecules that are used are ifosfamide and doxorubicin [ 11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Survival outcomes appear to be disappointing [ 32Miura J.T., Charlson J., Gamblin T.C., Eastwood D., Banerjee A., Johnston F.M., et al. Impact of chemotherapy on survival in surgically resected retroperitoneal sarcoma. Eur J Surg Oncol 2015 ; 41 (10) : 1386-1392 [cross-ref]], and data from the STRASS2 study evaluating neoadjuvant chemotherapy for grade 3 dedifferentiated liposarcoma and high-grade retroperitoneal leiomyosarcoma are awaited.
|
|
• |
In an adjuvant context, CT appears to have a benefit on local recurrence, but no studies have shown a benefit in overall survival specifically related to RPS [ 32Miura J.T., Charlson J., Gamblin T.C., Eastwood D., Banerjee A., Johnston F.M., et al. Impact of chemotherapy on survival in surgically resected retroperitoneal sarcoma. Eur J Surg Oncol 2015 ; 41 (10) : 1386-1392 [cross-ref], 33Italiano A., Delva F., Mathoulin-Pelissier S., Le Cesne A., Bonvalot S., Terrier P., et al. Effect of adjuvant chemotherapy on survival in FNCLCC grade 3 soft tissue sarcomas: a multivariate analysis of the French Sarcoma Group Database. Ann Oncol 2010 ; 21 (12) : 2436-2441 [cross-ref], 34Datta J., Ecker B.L., Neuwirth M.G., Geha R.C., Fraker D.L., Roses R.E., et al. Contemporary reappraisal of the efficacy of adjuvant chemotherapy in resected retroperitoneal sarcoma: Evidence from a nationwide clinical oncology database and review of the literature. Surg Oncol 2017 ; 26 (2) : 117-124 [cross-ref]].
|
|
• |
Hyperthermic intraperitoneal chemotherapy does not appear to provide a benefit for peritoneal Sarcomatosis compared to surgery, [ 35Bonvalot S., Cavalcanti A., Le Péchoux C., Terrier P., Vanel D., Blay J.Y., et al. Randomized trial of cytoreduction followed by intraperitoneal chemotherapy versus cytoreduction alone in patients with peritoneal Sarcomatosis. Eur J Surg Oncol 2005 ; 31 (8) : 917-923 [cross-ref]] but could have improved local control and relapse-free survival without an overall survival gain in a phase III study [ 15Pasquali S., Gronchi A. Neoadjuvant chemotherapy in soft tissue sarcomas: latest evidence and clinical implications. Ther Adv Med Oncol 2017 ; 9 (6) : 415-429 [cross-ref]].
|
|
• |
New drugs (TNF) and new routes of administration are being evaluated, which highlights the importance of including patients in trials. |
While metastatic RPSs are rare at the outset, approximately 1/3 of the cases follow a systemic course in their progression, which is often concomitant with local recurrence. In these contexts, CT has a palliative indication, for a modest benefit. The reference drugs are adriamycin, ifosfamide, doxorubicin, trabectidine and pazopanib. The objective response rate ranges from 16% to 29%, depending on the patient's general health and the tumour grade.
Table recommendation 1Treatment recommendations for RPSTreatment recommendations for RPSThe therapeutic strategy should be defined from initial care, coordinated by a sarcoma pathology reference centre± compartmental surgical excision is the cornerstone for treating localised or locally advanced forms of the diseaseMultimodal, adjuvant or neoadjuvant treatment, by radiotherapy or chemotherapy, optimises the oncological outcomes of high-risk tumours (but does not provide a survival benefit) and should be discussed in a referral MTMInclusion in therapeutic trials should be offered to patients with RPS in order to define the standards of treatment still under evaluationOverall survival and relapse-free survival are related to the quality of first-line management, including surgical excision, and the volume of cases treated per centre
| Table recommendation 1 - Treatment recommendations for RPS |
|
| Treatment recommendations for RPS |
| The therapeutic strategy should be defined from initial care, coordinated by a sarcoma pathology reference centre |
| ± compartmental surgical excision is the cornerstone for treating localised or locally advanced forms of the disease |
| Multimodal, adjuvant or neoadjuvant treatment, by radiotherapy or chemotherapy, optimises the oncological outcomes of high-risk tumours (but does not provide a survival benefit) and should be discussed in a referral MTM |
| Inclusion in therapeutic trials should be offered to patients with RPS in order to define the standards of treatment still under evaluation |
| Overall survival and relapse-free survival are related to the quality of first-line management, including surgical excision, and the volume of cases treated per centre |
|
The prognosis for RPS is generally poor. The quality of excision is the most significant prognostic factor in multivariate analysis (R2 21 months - median survival vs. R0/R1 69 months). The R2 character independently predicts the disease-specific mortality risk [36Tan M.CB., Brennan M.F., Kuk D., Agaram N.P., Antonescu C.R., Qin L.X., et al. Histology-based Classification Predicts Pattern of Recurrence and Improves Risk Stratification in Primary Retroperitoneal Sarcoma. Ann Surg 2016 ; 263 (3) : 593-600 [cross-ref]]. The volume of cases treated per centre is predictive of oncological outcomes [37Avancès C., Mottet N., Mahatmat A., Chapuis E., Serre I., Culine S. Prognostic factors for first recurrence in patients with retroperitoneal sarcoma. Urol Oncol 2006 ; 24 (2) : 94-96].
The overall survival rates at 5 and 10 years are 67 and 46%, local recurrence 26% and 35%, and metastatic dissemination 21% and 21.5% respectively [12Gronchi A., Strauss D.C., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann Surg 2016 ; 263 (5) : 1002-1009 [cross-ref]].
Many factors independently impact these numbers including age, tumour size, histological subtype, FLNCC grade, multifocality, and the quality of surgical excision. A nomogram integrating these data, which has been externally validated, is available, making it possible to include a prospective dimension in the therapeutic strategy [38Gronchi A., Miceli R., Shurell E., Eilber F.C., Eilber F.R., Anaya D.A., et al. Outcome prediction in primary resected retroperitoneal soft tissue sarcoma: histology-specific overall survival and disease-free survival nomograms built on major sarcoma center data sets. J Clin Oncol 2013 ; 31 (13) : 1649-1655 [cross-ref]].
Multimodal treatments complementary to surgery affect survival data differently according to histological subtypes. Therefore, well-differentiated fibrosarcoma is favourably impacted by adjuvant treatment for local recurrence, whereas leiomyosarcoma is not [12Gronchi A., Strauss D.C., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann Surg 2016 ; 263 (5) : 1002-1009 [cross-ref]].
Grade is a powerful independent prognostic factor for relapse-free survival (Table 4) [39Gronchi A., Miceli R., Allard M.A., Callegaro D., Le Péchoux C., Fiore M., et al. Personalizing the approach to retroperitoneal soft tissue sarcoma: histology-specific patterns of failure and postrelapse outcome after primary extended resection. Ann Surg Oncol 2015 ; 22 (5) : 1447-1454 [cross-ref]].
Local recurrence and its treatment are the main factors of disease-specific death in retroperitoneal sarcoma [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540,40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]]. The prognosis is generally poor for metastatic disease, including with the use of systemic therapies [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
Overall survival was reported at 33, 25 and 12 months after local, systemic and mixed recurrence, with 5-year survival rates of 29%, 20% and 14%. Therefore, the length of the time before recurrence is a major prognostic criterion [41MacNeill A.J., Miceli R., Strauss D.C., Bonvalot S., Hohenberger P., Van Coevorden F., et al. Post-relapse outcomes after primary extended resection of retroperitoneal sarcoma: A report from the Trans-Atlantic RPS Working Group. Cancer 2017 ; 123 (11) : 1971-1978 [cross-ref]].
The recommendations for surveillance are primarily based on the extrapolation of data acquired from the management of sarcomas of the extremities [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]].
The local recurrence rates reported by TARPSWG were 25.9% at 5 years and 35% at 10 years [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]], which supports surveillance of at least 10 years, and for some should be carried out for life [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]] due to recurrence after 15-20 years (without levelling) [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
The modalities of recurrence (period, multifocality, site), mainly local, are conditioned by the initial histological type and grade. Surveillance imaging is the main method of revealing recurrence since the symptoms remain non-specific for a long time [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]].
In patients with a complete response, CT-TAP scan with contrast injection is the reference examination. In case of well-differentiated/low grade liposarcoma, the metastatic risk being classically low or even nil, chest CT scan could be replaced by a simple chest X-ray with 2 views [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]].
Surveillance recommendations are not strictly consistent amongst learned societies. Some have not defined a specific protocol for the retroperitoneal location. It seems reasonable to suggest [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]]:
|
• |
For indolent histological forms (such as low grade/well differentiated liposarcoma): abdominal and pelvic CT scan every 6 months for 3 years and then annually. |
|
• |
For aggressive histological forms (such as dedifferentiated liposarcoma and intermediate to high grade leiomyosarcoma): thoraco-abdomino-pelvic CT scan every 3-4 months for 2 years then every 6 months for 3 years and then once a year. |
RPS is a rare tumour with which urologists are readily confronted as a first-line diagnosis. However, a key to the prognosis lies in the initial treatment. It is fundamental that the message of multidisciplinarity and coordination within a sarcoma reference network is heard and understood.
CCAFUFrench Urology Association Cancer CommitteeCTChemotherapyINCAFrench Cancer InstituteMRIMagnetic Resonance ImagingPCPPersonalised Care ProgramMTMMultidisciplinary Team MeetingRTRadiotherapyRPSRetroperitoneal Sarcoma18FDG PETPositron Emission Tomography
|
| CCAFU |
French Urology Association Cancer Committee |
| CT |
Chemotherapy |
| INCA |
French Cancer Institute |
| MRI |
Magnetic Resonance Imaging |
| PCP |
Personalised Care Program |
| MTM |
Multidisciplinary Team Meeting |
| RT |
Radiotherapy |
| RPS |
Retroperitoneal Sarcoma |
| 18FDG PET |
Positron Emission Tomography |
|
Les sarcomes du rétropéritoine (SRP) sont des tumeurs malignes rares (0,5 à 1 % des tumeurs malignes) [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref], 2Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20]. La localisation rétropéritonéale représente 12 à 15 % des sarcomes des tissus mous [3Toulmonde M., Bonvalot S., Méeus P., Stoeckle E., Riou O., Isambert N., et al. Retroperitoneal sarcomas: patterns of care at diagnosis, prognostic factors and focus on main histological subtypes: a multicenter analysis of the French Sarcoma Group. Ann Oncol 2014 ; 25 (3) : 735-742 [cross-ref]] et certains types histologiques y sont davantage représentés [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref]].
La grande majorité des SRP sont sporadiques, néanmoins 2 facteurs de risque sont identifiés [2Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20] :
|
• |
la radiothérapie, pourvoyeuse de sarcomes radio-induits (principalement histiocytofibromes malins, ostéosar-comes extra-squelettiques et fibrosarcomes) caractérisés par leur agressivité et leur pronostic sombre ; |
|
• |
plusieurs maladies héréditaires comme la neurofibromatose de type I (associée au schwannome malin), les altérations du gène RB ou la maladie de Li-Fraumeni (altération du gène suppresseur de tumeur TP53). |
La croissance des SRP s'effectue par poussées centrifuges successives qui délimitent une pseudo-capsule tumorale, toujours envahie et parfois franchie par des bourgeons tumoraux qui contaminent l'espace rétropéritonéal adjacent [2Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20]. Toute effraction de la pseudo-capsule (tumorectomie ou par biopsie chirurgicale) provoque une dissémination tumorale.
|
|
|
Diagnostic clinique (Figure 1)
|
|
|
|
|
|
Circonstances cliniques révélatrices
|
Les SRP sont de volume tumoral important au moment du diagnostic eu égard à l'espace dont ils disposent dans le rétropéritoine (RP) (18 cm de grand axe médian) [4Cates J.MM. Performance Analysis of the American Joint Committee on Cancer 8th Edition Staging System for Retroperitoneal Sarcoma and Development of a New Staging Algorithm for Sarcoma-Specific Survival. Ann Surg Oncol 2017 ; 24 (13) : 3880-3887 [cross-ref]].
Figure 1.
Démarche diagnostique du SRP.
En dehors des diagnostics fortuits sur une imagerie non dédiée, les douleurs (lombaire, abdominale) et les compressions urétérales ou du grêle sont les principales circonstances diagnostiques. La découverte de telles tumeurs doit faire suspecter l'existence d'un SRP jusqu'à la preuve histologique du contraire.
L'extension à distance est rare lors du primo-diagnostic mais reste possible, notamment en situation de rechute ou lorsqu'il s'agit d'un léiomyosarcome de haut grade.
Scanner thoraco-abdomino-pelvien (TDM TAP)
La TDM TAP avec injection de produit de contraste est indispensable à la démarche diagnostique et à l'élaboration du projet thérapeutique :
|
• |
Évoquer le diagnostic positif : devant une lésion localisée au rétropéritoine, non développée aux dépens d'un organe. Le caractère rétropéritonéal est parfois difficile à évaluer lorsque les masses sont volumineuses mais le déplacement des organes rétropéritonéaux est un indice utile. La tumeur peut franchir des défilés anatomiques, ce qui est caractéristique du mode de développement. Le SRP n'a classiquement pas d'artère nourricière. |
|
• |
Évoquer dans certains cas la nature histologique : les liposarcomes peuvent avoir une composante de densité graisseuse et comporter des cloisons vascularisées. La disparition de la veine cave inférieure est quant à elle un signe évocateur d'un sarcome de la veine cave (léiomyosarcome, angiosarcome). |
|
• |
Planifier la procédure biopsique de la tumeur primitive ou d'une métastase. |
|
• |
Réaliser le bilan d'extension ganglionnaire et systémique (jusqu'à 50% de métastases pulmonaires au diagnostic de léiomyosarcome). |
|
• |
Étudier les critères de résécabilité [ 5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]].
|
L'IRM abdominale sera indiquée chez le patient allergique aux produits de contrastes iodés, en complément d'un scanner sans injection, ou dans les cas d'analyse difficile au scanner. L'extension musculaire, osseuse, foraminale, ou vasculaire pourra ainsi être mieux précisée. Dans le pelvis, l'IRM peut être utile pour délimiter la lésion.
Le protocole d'IRM inclut des séquences classiques T1 et T2, des séquences avec saturation de graisse, des séquences de diffusion et des séquences dynamiques après injection de gadolinium. L'antenne corps permet d'étudier les limites de la tumeur dans tous les plans.
Lorsque la radiothérapie est considérée, elle permet de délimiter le volume de traitement, qui pour être optimal inclura l'Ådème péritumoral [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]].
L'échographie ne permet pas d'éliminer le diagnostic, mais peut permettre la découverte initiale d'une masse amorçant la démarche diagnostique.
La TEP-18FDG n'est pas indiquée dans le diagnostic initial étant donné la variabilité des types histologiques et grades rencontrés. Elle n'est pas assez discriminante pour distinguer les sarcomes de bas grade des tumeurs bénignes [5]. Elle peut néanmoins trouver une place dans le suivi évolutif d'une tumeur en récidive eu égard à sa sensibilité et sa spécificité supérieures à celles du scanner dans cette situation, ou dans l'évaluation des formes agressives [6Roberge D., Vakilian S., Alabed Y.Z., Turcotte R.E., Freeman C.R., Hickeson M. FDG PET/CT in Initial Staging of Adult Soft-Tissue Sarcoma. Sarcoma 2012 ; 2012 : 960194].
La scintigraphic osseuse peut trouver un intérêt dans le diagnostic différentiel d'une tumeur primitive osseuse à extension de contiguïté aux parties molles adjacentes.
Dans les cas où l'exérèse concernera un des reins, une évaluation biologique et par scintigraphic à l'acide dimercaptosuccinique (DMSA) de la fonction rénale est recommandée, permettant d'anticiper une éventuelle prise en charge néphrologique [7].
|
|
|
Démarche diagnostique (Figure 1)
|
|
|
Dès lors que le SRP est suspecté, et avant la réalisation de la biopsie, le dossier doit être discuté en réunion de concertation pluridisciplinaire (RCP) spécialisée. Le réseau français de référence en pathologie des sarcomes (RRePS-TMV) peut être sollicité, comprenant 3 centres coordonnateurs et 19 centres référents (www.infosarcomes.org) répartis sur le territoire national.
Cette attitude permet de confirmer le degré de suspicion, d'optimiser la biopsie (rendement et sécurité contre la dissémination), de planifier et d'anticiper la stratégie thérapeutique obligatoirement multidisciplinaire, souvent multimodale et, dans tous les cas, hautement spécialisée.
Bien qu'évoqué à l'imagerie, le diagnostic positif sera histo-logique, par la biopsie. Cette attitude permet de redresser plusieurs diagnostics différentiels parmi lesquels les tumeurs bénignes, les tumeurs germinales extra-gonadiques, les lymphomes [5,8]. Les SRP ne représentent qu'un tiers des tumeurs rétropéritonéales [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
La biopsie percutanée radiologique est réalisée par voie extra-péritonéale sur un trajet court, en mandrin protégé (aiguille coaxiale) [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref], 8Van Houdt W.J., Schrijver A.M., Cohen-Hallaleh R.B., Memos N., Fotiadis N., Smith M.J., et al. Needle tract seeding following core biopsies in retroperitoneal sarcoma. Eur J Surg Oncol 2017 ; 43 (9) : 1740-1745 [cross-ref]]. Elle est actuellement le standard de prélèvement [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
Le guidage par scanner aide à choisir le trajet et une zone d'intérêt tissulaire (hors nécrose et zone kystique, de préférence dans la portion la moins adipeuse) [5]. Lorsque techniquement et raisonnablement possible, le prélèvement doit concerner différentes zones. Le diamètre de l'aiguille est choisi par le radiologue, en fonction du trajet, des risques hémorragiques : une aiguille de 18 ou mieux 16G permet en général un diagnostic histologique. Le risque de contamination du trajet est faible bien qu'existant et il ne semble pas être associé à davantage de récidive locale [8]. Le trajet peut être tatoué pour repérage ultérieur permettant l'excision [7Casali P.G., Abecassis N., Bauer S., Biagini R., Bielack S., Bonvalot S., et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 28 mai 2018 ; 29 : iv51-67]. Lorsque le diagnostic n'était pas attendu, le trajet biopsique pourrait être concerné par l'acte chirurgical d'exérèse.
Il a été recommandé d'adresser un prélèvement à l'état frais au laboratoire d'anatomie pathologique pour envisager une congélation en fonction de l'abondance de matériel biopsique et permettre la réalisation ultérieure de tests moléculaires [7Casali P.G., Abecassis N., Bauer S., Biagini R., Bielack S., Bonvalot S., et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 28 mai 2018 ; 29 : iv51-67]. Désormais les études moléculaires peuvent être assurées sur tissus fixés en formol et inclus en paraffine.
La biopsie chirurgicale peut fournir davantage de matériel mais son indication doit être balancée par le risque d'essaimage résultant de l'effraction de la pseudo-capsule. Elle relève d'une décision de centre de référence [7]. Elle doit être strictement extra-péritonéale. La voie d'abord doit être réséquée lors du traitement définitif. Les voies transsphinctérienne et transvaginale doivent être proscrites eu égard à l'affinité des récidives pour les cicatrices qui péjore dans ces situations le pronostic fonctionnel.
Quelle que soit la modalité de prélèvement, l'approche transpéritonéale doit être le dernier recours diagnostique, après discussion du dossier en concertation pluridisciplinaire spécialisée [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]].
L'analyse histologique définitive relèvera d'un pathologiste spécialisé [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
Les SRP sont classés en fonction de leur ressemblance au tissu mésenchymateux d'origine.
Le liposarcome est la forme histologique la plus fréquente (30 à 60% des cas) [5,11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Il s'agit d'une tumeur localement agressive composée de tissu adipeux. Le liposarcome est sous-divisé en forme bien différenciée (45,8 % des cas), indifférenciées (44,8 %), myxoïde (4,7 %) et pléomorphe (0,8%) [11]. Les formes indifférenciées y associent une composante non adipocytaire de haut grade. Dans les cas douteux, le diagnostic histologique est conforté par la mise en évidence d'une amplification du gène murine double minute 2 (MDM2) par hybridation in situ fluorescente (FISH) ou colorimétrique (CISH). Les lipomes (bénins) étant extrêmement rares dans le rétropéritoine, le diagnostic ne devrait pas être posé sans cette évaluation. La forme dédifférenciée est à l'inverse très fréquente dans le rétropéritoine et peut également être retrouvée au niveau du cordon spermatique [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref]].
Le léiomyosarcome (20 à 30 % des cas) comprend des cellules à différenciation musculaire lisse [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref],11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Les localisations rétropéritonéales et pelviennes sont les plus fréquentes. Une masse développée aux dépens d'un vaisseau du rétropéritoine (veine cave inférieure, aorte, vaisseaux gonadiques notamment) est évocatrice [11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Les léiomyosarcomes sont parmi les sarcomes biologiquement les plus agressifs et sont caractérisés par un haut taux de mortalité [1Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref]]. Leur dissémination métastatique est principalement hématogène [12Gronchi A., Strauss D.C., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann Surg 2016 ; 263 (5) : 1002-1009 [cross-ref]].
Le terme « histiocytofibrome malin » représentait moins de 10% des cas [11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. La plupart des diagnostics d'HFM se sont révélés finalement appartenir à un autre sous-type histologique indifférencié, souvent liposarcome. En pratique, ce terme ne devrait plus être employé.
Les autres sarcomes sont plus rares : fibrosarcome, rhabdomyosarcome, synovialosarcome, sarcome d'Ewing ou schwannome malin [11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]].
Les principaux critères pronostiques sont la taille, le type histologique et le grade selon les critères définis par la Fédération nationale des centres de lutte contre le cancer (FNCLCC).
Les léiomyosarcomes et les angiosarcomes sont des tumeurs agressives pour lesquelles le grade histologique n'est pas un critère discriminant. Par ailleurs, quel que soit le sous-type histologique, les critères pris en compte pour définir le grade FNCLCC sont l'index mitotique, la différenciation cellulaire et la nécrose tumorale.
La somme de chacun des critères permet d'établir un score qui varie de 2 à 8, traduit en 3 grades (Tableau 1) [13Trojani M., Contesso G., Coindre J.M., Rouesse J., Bui N.B., de Mascarel A., et al. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int J Cancer 1984 ; 33 (1) : 37-42 [cross-ref]].
La classification TNM des sarcomes du rétropéritoine est principalement déterminée par la taille tumorale [14] (Tableau 2). Cette classification est l'objet de critiques, notamment en ce qui concerne le stade T car la taille médiane au diagnostic classe la majorité des SRP en stade T4, malgré une sous-division plus importante de la taille dans sa dernière actualisation [15Pasquali S., Gronchi A. Neoadjuvant chemotherapy in soft tissue sarcomas: latest evidence and clinical implications. Ther Adv Med Oncol 2017 ; 9 (6) : 415-429 [cross-ref]]. La taille tumorale, en tant que variable continue, a un effet modeste sur la survie (HR 1,004 ; p = 0,04) contrairement au stade T4 (HR 1,3 ; p < 0,001) qui reste un facteur pronostique moins puissant que le haut grade (HR 2,5 ; p < 0,001) ou la résection macroscopiquement incomplète R2 (HR 1,97 ; p < 0,001) [16Fisher S.B., Chiang Y-J, Feig B.W., Cormier J.N., Hunt K.K., Torres K.E., et al. An Evaluation of the Eighth Edition of the American Joint Committee on Cancer (AJCC) Staging System for Retroperitoneal Sarcomas Using the National Cancer Data Base (NCDB): Does Size Matter?. Am J Clin Oncol 2019 ; 42 (2) : 160-165 [cross-ref]].
Les stades AJCC sont définis par synthèse du stade TNM et du grade FNCLCC [14] (Tableau 3). Cette stadification simple pourrait être insuffisante et l'évaluation du pronostic serait davantage discriminante en tenant compte : de la taille tumorale, du type histologique (favorable/défavorable) et du grade FNCLCC [4Cates J.MM. Performance Analysis of the American Joint Committee on Cancer 8th Edition Staging System for Retroperitoneal Sarcoma and Development of a New Staging Algorithm for Sarcoma-Specific Survival. Ann Surg Oncol 2017 ; 24 (13) : 3880-3887 [cross-ref]]. De multiples nomogrammes ont été développés, dont certains spécifiques du sarcome rétropéritonéal [17Callegaro D., Miceli R., Gladdy R.A. Prognostic models for RPS patients-Attempting to predict patient outcomes. J Surg Oncol 2018 ; 117 (1) : 69-78 [cross-ref]].
|
|
|
|
|
Chirurgie à visée curative
|
Pierre angulaire du traitement à visée curative, la chirurgie d'exérèse des SRP répond à des impératifs carcinologiques de qualité d'exérèse et à des exigences techniques de résécabilité. Une résection macroscopiquement complète améliore la survie bien que le taux de récidive locale demeure globalement élevé [9]. Dans ces conditions, avec un volume tumoral médian important et des gestes combinés courants, la discussion de la voie d'abord est actuellement restreinte, les rares études laparoscopiques étant biaisées par un volume d'exérèse limité et un suivi insuffisant [18Gronchi A., Crago A., Raut C.P. Minimally Invasive Surgery for Retroperitoneal Sarcoma: Just Because We Can Does Not Mean We Should. Ann Surg Oncol 2018 ; 25 (8) : 2129-2131 [cross-ref]].
Figure 2.
Démarche thérapeutique du SRP localisé.
|
| Impératifs carcinologiques |
L'objectif carcinologique est la résection monobloc de la tumeur en marge saine microscopique (R0), ce d'autant qu'il n'existe aucun traitement de rattrapage systémique d'une chirurgie macroscopiquement incomplète et que l'effraction tumorale favorise la dissémination péritonéale (sarcomatose). La pseudo-capsule qui entoure le sarcome est constituée d'un front de cellules tumorales densifiées qui ne représente pas un plan de clivage pertinent.
La notion de chirurgie compartimentale est dérivée des principes des sarcomes des extrémités pour lesquels une marge de muscle sain enveloppant la tumeur est systématiquement prélevée [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
Elle constitue l'exérèse d'un quadrant abdominal emportant au moins les organes refoulés et parfois les organes au contact [19]. Cela est particulièrement vrai pour l'intestin grêle et le tractus urinaire supérieur. Un geste orthopédique peut être nécessaire pour l'exposition très large peut être indiqué pour l'exposition très large nécessaire à cette chirurgie compartimentale monobloc (rachis, sacrum).
Une étude rétrospective des chirurgies compartimentales a rapporté un envahissement histologique de 65 % des organes suspects d'être envahis, 26 % des organes adhérents, 19 % des organes enveloppés mais aucun des autres organes faisant partie de la résection en bloc [20Fairweather M., Wang J., Jo V.Y., Baldini E.H., Bertagnolli M.M., Raut C.P. Surgical Management of Primary Retroperitoneal Sarcomas: Rationale for Selective Organ Resection. Ann Surg Oncol 2018 ; 25 (1) : 98-106 [cross-ref]].
Si cette chirurgie a pour objectif d'atteindre des marges de résection macroscopiquement saines, elle expose à une morbidité plus importante, en particulier lorsque le duodénum, les gros vaisseaux, le pancréas ou des nerfs majeurs sont impliqués [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
Il s'agit d'une chirurgie difficile, techniquement complexe relevant d'une équipe multidisciplinaire. La morbidité est importante, y compris dans des centres de référence, avec 16,4 % de complications Clavien-Dindo ⥠3 (notamment en cas de résection vasculaire majeure ou chirurgie pancréatique) et 1,8 % de décès à 30 jours [21MacNeill A.J., Gronchi A., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Postoperative Morbidity After Radical Resection of Primary Retroperitoneal Sarcoma: A Report From the Transatlantic RPS Working Group. Ann Surg 2018 ; 267 (5) : 959-964 [cross-ref]].
Une équipe multidisciplinaire dédiée semble indispensable à l'élaboration du plan thérapeutique et à sa mise en Åuvre avec la moindre morbidité [22Maurice M.J., Yih J.M., Ammori J.B., Abouassaly R. Predictors of surgical quality for retroperitoneal sarcoma: Volume matters. J Surg Oncol 2017 ; 116 (6) : 766-774 [cross-ref]].
En l'absence d'étude randomisée évaluant le bénéfice de la chirurgie large, certains évoquent le recours à une stratégie reposant sur des données anatomiques et histo-logiques, les patients pouvant le plus bénéficier de cette chirurgie étant ceux porteurs d'un sous-type agressif comme le liposarcome dédifférencié de haut grade [9]. Dans d'autres histologies [23], une chirurgie R0 large pourrait être suffisante, correspondant à une résection en marge saine avec un liseré de tissu sain sans sacrifice d'organe systématique.
En France, une étude rétrospective observait un taux de chirurgie R0 de 41,9 % dans les centres du réseau NetSarc (volume médian de 2010 à 2017 : 23 cas [3-209]) contre 12,3 % dans les centres hors du réseau (volume médian : 1 cas [1-2]) [24Bonvalot S., Gaignard E., Stoeckle E., Meeus P., Decanter G., Carrere S., et al. Survival Benefit of the Surgical Management of Retroperitoneal Sarcoma in a Reference Center: A Nationwide Study of the French Sarcoma Group from the NetSarc Database. Ann Surg Oncol 2019 ; 26 (7) : 2286-2293 [cross-ref]].
Les possibilités techniques d'exérèse chirurgicale ou résécabilité de la tumeur influent lourdement la stratégie thérapeutique. L'expertise d'un centre référent est particulièrement requise afin d'évaluer le risque vital périopératoire et la profondeur du préjudice fonctionnel (longueur du grêle, tractus urogénital).
Le taux de résécabilité des tumeurs atteint aujourd'hui 80 %. Le principal critère de non-résécabilité de la tumeur est l'engainement circulaire de l'artère mésentérique supérieure. A contrario , l'extension intrarachidienne par un trou de conjugaison, l'envahissement ou l'extension circonférentielle de l'aorte, l'envahissement de la veine cave, le caractère pan abdominal nécessitent des adaptations techniques permettant une résection dans des conditions acceptables.
|
|
|
Chirurgie de seconde intention
|
La récidive locale survient dans 22 à 84 % des cas en fonction du sous-type histologique, du grade et de la qualité de l'exérèse initiale [9Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref]].
Si 85 % des SRP opérés en intention curative peuvent aboutir à une résection macroscopiquement complète (R0/R1) lors de la première chirurgie, ce taux est inférieur à 50 % en chirurgie de seconde intention [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
La résection R0 d'une récidive de SRP peut être interprétée comme la seule option curative mais les chances limitées de survie sans progression doivent être identifiées par la RCP pour balancer l'indication de chirurgie large avec sacrifice d'organe/fonction [10]. La morbi-mortalité est importante, aussi l'évaluation de l'état général du patient est un critère important de sélection [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540] afin d'éviter une altération de la qualité de vie lorsque la guérison ne sera pas assurée [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
La probabilité de résection complète réduit avec le nombre de récidive et la notion de morcellation dans le champ de la tumeur initiale [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]]. Le pronostic s'aggrave avec le nombre de nodules de carcinose péritonéale [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
Un traitement néo-adjuvant peut être indiqué particulièrement dans les cas de léiomyosarcome, liposarcome dédifférencié, sarcome pléomorphe, tumeurs fibreuses solitaires et synovialosarcome [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
Les métastases viscérales sont présentes dans 10-20 % des cas au diagnostic et constituent rarement le site de première récidive de la maladie [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]]. La métastasectomie pourrait présenter un bénéfice de survie chez certains patients oligométastatiques sélectionnés [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540]. L'exérèse chirurgicale des métastases pulmonaires, quel qu'en soit le nombre, a montré un bénéfice en survie [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]], ce qui n'est pas le cas pour les métastases hépatiques où la chirurgie n'est pas le standard [19Bonvalot S., Raut C.P., Pollock R.E., Rutkowski P., Strauss D.C., Hayes A.J., et al. Technical considerations in surgery for retroperitoneal sarcomas: position paper from E-Surge, a master class in sarcoma surgery, and EORTC-STBSG. Ann Surg Oncol 2012 ; 19 (9) : 2981-2991 [cross-ref]].
En présence d'une récidive synchrone abdominale et à distance, le traitement systémique doit être considéré en premier au sein d'une approche multimodale [9, 10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540].
L'intérêt de l'adjonction de la radiothérapie est soutenu par un faible niveau de preuve et repose essentiellement sur l'extrapolation des résultats démontrés pour le contrôle local des sarcomes des extrémités de haut grade, avec parfois des technologies d'irradiation anciennes [26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. La localisation rétropéritonéale, la proximité de structures radiosensibles compliquent les modalités d'irradiation.
Le moment de la radiothérapie est sujet à controverse :
|
• |
La radiothérapie néo-adjuvante repose sur l'optimisation théorique de l'oxygénation tissulaire avant chirurgie, un contourage plus aisé, l'intérêt du refoulement des organes radiosensibles par la tumeur, et un niveau de dose plus faible qu'en adjuvant. La dose recommandée est de 50-50,4 Gy en fractions de 1,8-2 Gy et des boosts peuvent être additionnés sur les zones à risque de marges positives [ 26]. La chirurgie sera proposée 4 à 8 semaines après la fin de la radiothérapie. Des études rétrospectives sont favorables à cette modalité en ce qui concerne la survie globale mais ne livrent pas tous les détails attendus concernant notamment la récidive et la toxicité [ 26]. Une méta-analyse récente est en faveur d'un bénéfice en survie sans progression et globale de la radiothérapie périopératoire en comparaison à la chirurgie seule, davantage marquée en néo-adjuvant [ 27Diamantis A., Baloyiannis I., Magouliotis D.E., Tolia M., Symeonidis D., Bompou E., et al. Perioperative radiotherapy versus surgery alone for retroperitoneal sarcomas: a systematic review and meta-analysis. Radiol Oncol 2020 ; 54 (1) : 14-21 [cross-ref]]. Une étude rétrospective du TARPSWG ne confirme pas cet avantage après ajustement statistique [ 28Haas R.LM., Bonvalot S., Miceli R., Strauss D.C., Swallow C.J., Hohenberger P., et al. Radiotherapy for retroperitoneal liposarcoma: A report from the Transatlantic Retroperitoneal Sarcoma Working Group. Cancer 2019 ; 125 (8) : 1290-1300 [cross-ref]]. L'étude randomisée prospective EORTC STRASS (NCT01344018), dont les inclusions sont terminées depuis 2018, randomisait les patients atteints de SRP non métastatique entre chirurgie seule et radiothérapie néo-adjuvante puis chirurgie. L'objectif principal est la survie sans récidive intra-abdominale. Ses résultats, toujours en attente, seront déterminants dans les indications futures de radiothérapie.
|
|
• |
La radiothérapie adjuvante postopératoire concerne tout ou partie du champ opératoire, pouvant être repéré par des clips chirurgicaux. Les données de survie globale provenant de la base Surveillance, Epidemiology, and End Results (SEER) sont contradictoires [ 26, 29]. La principale limite est la morbidité tardive, rapportée entre 5 et 40 % des cas pour des doses de 50 à 60 Gy [ 26]. L'utilisation de « spacers » (notamment de prothèses mammaires, pour éloigner les anses intestinales de la zone à irradier) a été rapportée, non sans morbidité [ 26]. Le recours à la chirurgie première large et à la radiothérapie néo-adjuvante a drastiquement réduit les indications de traitement [ 30Almond L.M., Gronchi A., Strauss D., Jafri M., Ford S., Desai A. Neoadjuvant and adjuvant strategies in retroperitoneal sarcoma. Eur J Surg Oncol 2018 ; 44 (5) : 571-579 [cross-ref]].
|
|
• |
Les résultats de la curiethérapie et de la radiothérapie peropératoire ont été mitigés et associés à une morbidité significative [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]]. Le taux de complications digestives doit d'ailleurs faire renoncer à la curiethérapie dans la partie haute de l'abdomen [ 31Naghavi A.O., Fernandez D.C., Mesko N., Juloori A., Martinez A., Scott J.G., et al. American Brachytherapy Society consensus statement for soft tissue sarcoma brachytherapy. Brachytherapy 2017 ; 16 (3) : 466-489 [cross-ref]].
|
|
• |
Des thérapies émergentes (protons, ions carbone) sont développées afin d'améliorer l'efficacité et de réduire la radiotoxicité de ces modalités adjuvantes [ 26Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref]].
|
Au total, la radiothérapie en traitement multimodal associée à la chirurgie semblerait pouvoir améliorer le contrôle local, selon certaines modalités (plutôt préopératoire) et pour certaines tumeurs (bien circonscrites, haut grade) qui nécessitent d'être mieux identifiées par l'inclusion dans des essais prospectifs.
Le rationnel de l'utilisation de la chimiothérapie (CT) périopératoire dans le SRP s'appuie sur des notions telles que la cytoréduction préopératoire, la stérilisation micro-métastatique, l'évaluation de la chimio-sensibilité sur les spécimens de résection :
|
• |
En situation néo-adjuvante, la CT permet d'obtenir des réponses objectives (à l'exception du liposarcome bien différencié non chimio-sensible) de l'ordre de 21-33 %, notamment sur le volume tumoral [ 11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Elle est discutée pour de larges tumeurs de haut grade, notamment lorsqu'une néphrectomie associée est anticipée mais le faible taux de réponse ne doit pas faire retarder la chirurgie complète d'une masse résécable [ 15Pasquali S., Gronchi A. Neoadjuvant chemotherapy in soft tissue sarcomas: latest evidence and clinical implications. Ther Adv Med Oncol 2017 ; 9 (6) : 415-429 [cross-ref]]. Les molécules classiquement utilisées sont l'ifosfamide et la doxorubicine [ 11Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref]]. Les résultats en survie semblent décevants, et on attend les données de l'étude STRASS2 évaluant la CT néo-adjuvante des liposarcomes dédifférenciés de grade 3 et des léiomyosarcomes de haut grade du rétropéritoine [ 32Miura J.T., Charlson J., Gamblin T.C., Eastwood D., Banerjee A., Johnston F.M., et al. Impact of chemotherapy on survival in surgically resected retroperitoneal sarcoma. Eur J Surg Oncol 2015 ; 41 (10) : 1386-1392 [cross-ref]].
|
|
• |
En situation adjuvante, la CT semble apporter un bénéfice sur la récidive locale, mais aucune étude n'a montré de bénéfice en survie globale concernant spécifiquement le SRP [ 32Miura J.T., Charlson J., Gamblin T.C., Eastwood D., Banerjee A., Johnston F.M., et al. Impact of chemotherapy on survival in surgically resected retroperitoneal sarcoma. Eur J Surg Oncol 2015 ; 41 (10) : 1386-1392 [cross-ref], 33Italiano A., Delva F., Mathoulin-Pelissier S., Le Cesne A., Bonvalot S., Terrier P., et al. Effect of adjuvant chemotherapy on survival in FNCLCC grade 3 soft tissue sarcomas: a multivariate analysis of the French Sarcoma Group Database. Ann Oncol 2010 ; 21 (12) : 2436-2441 [cross-ref], 34Datta J., Ecker B.L., Neuwirth M.G., Geha R.C., Fraker D.L., Roses R.E., et al. Contemporary reappraisal of the efficacy of adjuvant chemotherapy in resected retroperitoneal sarcoma: Evidence from a nationwide clinical oncology database and review of the literature. Surg Oncol 2017 ; 26 (2) : 117-124 [cross-ref]].
|
|
• |
La CT hyperthermique intrapéritonéale ne semble pas apporter de bénéfice par rapport à la chirurgie dans les cas de sarcomatose péritonéale [ 35Bonvalot S., Cavalcanti A., Le Péchoux C., Terrier P., Vanel D., Blay J.Y., et al. Randomized trial of cytoreduction followed by intraperitoneal chemotherapy versus cytoreduction alone in patients with peritoneal Sarcomatosis. Eur J Surg Oncol 2005 ; 31 (8) : 917-923 [cross-ref]] mais aurait apporté une amélioration du contrôle local et de la survie sans récidive sans gain de survie globale dans une étude de phase III [ 15Pasquali S., Gronchi A. Neoadjuvant chemotherapy in soft tissue sarcomas: latest evidence and clinical implications. Ther Adv Med Oncol 2017 ; 9 (6) : 415-429 [cross-ref]].
|
|
• |
De nouvelles drogues (TNF), de nouvelles voies d'administration sont en cours d'évaluation, rappelant l'importance de l'inclusion des patients dans les essais. |
Si le SRP d'emblée métastatique est rare, environ un tiers des cas connaissent une évolution systémique au décours de leur évolution, volontiers concomitante d'une récidive locale. Dans ces situations, la CT trouve une indication palliative, pour un bénéfice modeste. Les drogues de références sont l'adriamycine, l'ifosfamide, la doxorubicine, la trabectédine et le pazopanib. Le taux de réponse objective oscille entre 16 et 29 %, selon l'état général du patient et le grade tumoral.
Tableau de recommandation 1Recommandations thérapeutiques pour le SRPLa stratégie thérapeutique doit être définie dès la prise en charge initiale, coordonnée par centre de référence en pathologie du sarcomeLa chirurgie d'exérèse ± compartimentale est la pierre angulaire du traitement des formes localisées ou localement avancéesLe traitement multimodal, adjuvant ou néo-adjuvant, par radiothérapie ou chimiothérapie, optimise les résultats carcinologiques des tumeurs à haut risque (sans toutefois apporter de bénéfice en survie) et doit être discuté au sein d'une RCP référenteL'inclusion dans des essais thérapeutiques doit être proposée aux patients atteints de SRP afin de définir les standards de traitement encore en évaluationLa survie globale et la survie sans récidive sont liées à la qualité de la prise en charge de première intention, notamment de l'exérèse chirurgicale, ainsi qu'au volume de cas traité par centre.
|
| Recommandations thérapeutiques pour le SRP |
| La stratégie thérapeutique doit être définie dès la prise en charge initiale, coordonnée par centre de référence en pathologie du sarcome |
| La chirurgie d'exérèse ± compartimentale est la pierre angulaire du traitement des formes localisées ou localement avancées |
| Le traitement multimodal, adjuvant ou néo-adjuvant, par radiothérapie ou chimiothérapie, optimise les résultats carcinologiques des tumeurs à haut risque (sans toutefois apporter de bénéfice en survie) et doit être discuté au sein d'une RCP référente |
| L'inclusion dans des essais thérapeutiques doit être proposée aux patients atteints de SRP afin de définir les standards de traitement encore en évaluation |
| La survie globale et la survie sans récidive sont liées à la qualité de la prise en charge de première intention, notamment de l'exérèse chirurgicale, ainsi qu'au volume de cas traité par centre |
|
Le pronostic des SRP est globalement péjoratif. La qualité d'exérèse est le facteur pronostique le plus significatif en analyse multivariée (R2 21 mois de survie médiane vs R0/R1 69 mois). Le caractère R2 prédit indépendamment le risque de mortalité spécifique [36Tan M.CB., Brennan M.F., Kuk D., Agaram N.P., Antonescu C.R., Qin L.X., et al. Histology-based Classification Predicts Pattern of Recurrence and Improves Risk Stratification in Primary Retroperitoneal Sarcoma. Ann Surg 2016 ; 263 (3) : 593-600 [cross-ref]]. Le volume de cas traités par centre est prédictif des suites oncologiques [37Avancès C., Mottet N., Mahatmat A., Chapuis E., Serre I., Culine S. Prognostic factors for first recurrence in patients with retroperitoneal sarcoma. Urol Oncol 2006 ; 24 (2) : 94-96].
Les taux de survie globale à 5 et 10 ans sont de 67 et 46 %, de récidive locale de 26 et 35 %, de dissémination métastatique de 21 et 21,5 % respectivement [12Gronchi A., Strauss D.C., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann Surg 2016 ; 263 (5) : 1002-1009 [cross-ref]].
De nombreux facteurs impartent de manière indépendante ces chiffres parmi lesquels l'âge, la taille de la tumeur, le sous-type histologique, le grade FLNCC, la multifocalité et la qualité de l'exérèse chirurgicale. Un nomogramme tenant compte de ces données, et ayant fait l'objet d'une validation externe, est disponible, permettant d'intégrer à la stratégie thérapeutique une dimension prospective [38Gronchi A., Miceli R., Shurell E., Eilber F.C., Eilber F.R., Anaya D.A., et al. Outcome prediction in primary resected retroperitoneal soft tissue sarcoma: histology-specific overall survival and disease-free survival nomograms built on major sarcoma center data sets. J Clin Oncol 2013 ; 31 (13) : 1649-1655 [cross-ref]].
Les traitements multimodaux complémentaires à la chirurgie influent les données de survie diversement en fonction des sous-types histologiques. Ainsi, le fibrosarcome bien différencié est favorablement impacté par un traitement adjuvant pour la récidive locale, alors que le leiomyosarcome ne l'est pas [12Gronchi A., Strauss D.C., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann Surg 2016 ; 263 (5) : 1002-1009 [cross-ref]].
Le grade est un puissant facteur pronostique indépendant de survie sans récidive (Tableau 4) [39Gronchi A., Miceli R., Allard M.A., Callegaro D., Le Péchoux C., Fiore M., et al. Personalizing the approach to retroperitoneal soft tissue sarcoma: histology-specific patterns of failure and postrelapse outcome after primary extended resection. Ann Surg Oncol 2015 ; 22 (5) : 1447-1454 [cross-ref]].
La récidive locale et son traitement sont les facteurs principaux de décès spécifique dans le sarcome rétropéritonéal [10Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540, 40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]]. Le pronostic est globalement sombre en cas d'atteinte métastatique, y compris en ayant recours aux thérapies systémiques [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
La survie globale a été rapportée à 33, 25 et 12 mois après récidive locale, systémique et mixte, soit des taux de survie à 5 ans de 29, 20 et 14 %. La durée de l'intervalle avant récidive est alors un critère pronostique majeur [41MacNeill A.J., Miceli R., Strauss D.C., Bonvalot S., Hohenberger P., Van Coevorden F., et al. Post-relapse outcomes after primary extended resection of retroperitoneal sarcoma: A report from the Trans-Atlantic RPS Working Group. Cancer 2017 ; 123 (11) : 1971-1978 [cross-ref]].
Les recommandations de suivi se fondent principalement sur l'extrapolation des données acquises de la prise en charge des sarcomes des extrémités [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]].
Les taux de récidive locale rapportés par le TARPSWG étaient de 25,9 % à 5 ans et 35 % à 10 ans [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]] confortant un suivi d'au moins 10 ans, qui pour certains doit être réalisé à vie [5Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref]] du fait de l'existence de récidives après 15-20 ans (sans atteindre de plateau) [25Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref]].
Les modalités de récidives (délai, multifocalité, site), principalement locales, sont conditionnées par le type histologique initial et le grade. L'imagerie de suivi est le principal mode de révélation de la récidive dans la mesure où les symptômes sont longtemps aspécifiques [40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]].
Chez un patient en réponse complète, la TDM TAP avec injection de produit de contraste est l'examen de référence. En cas de liposarcome bien différencié/bas grade, le risque métastatique étant classiquement faible, voire nul, le scanner thoracique pourrait être remplacé par une simple radiographie thoracique en 2 incidences [40].
Les recommandations de suivi ne sont pas strictement concordantes selon les sociétés savantes. Certaines n'ont pas défini de protocole spécifique à la localisation rétropéritonéale. Il semble raisonnable de proposer :
|
• |
pour les formes histologiques indolentes (comme le liposarcome de bas grade/bien différencié) : scanner abdominopelvien tous les 6 mois pendant 3 ans puis annuel ; |
|
• |
pour les formes histologiques agressives (comme le liposarcome dédifférencié et le léiomyosarcome de grade intermédiaire à haut) : scanner TAP tous les 3-4 mois pendant 2 ans puis tous les 6 mois pendant 3 ans puis une fois par an [ 40Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref]].
|
Le SRP est une tumeur rare à laquelle les urologues sont volontiers confrontés en première intention diagnostique. Or, une clé du pronostic réside dans la prise en charge initiale. Il est fondamental que le message de multidisciplinarité et de coordination au sein d'un réseau référent sarcome soit entendu et compris.
|
| CCAFU |
Comité de cancérologie de l'Association française d'urologie |
| CT |
Chimiothérapie |
| INCA |
Institut national du cancer |
| IRM |
Imagerie par résonance magnétique |
| PPS |
Programme personnalisé de soins |
| RCP |
Réunion de concertation pluridisciplinaire |
| RT |
Radiothérapie |
| SRP |
Sarcome rétropéritonéal |
| TEP-18FDG |
Tomographie par émission de positons |
|
|
|
|
Déclaration de liens d'intérêts
|
P.-H. Savoie : Orateur et consultant pour le CCAFU online (AFU), Consultant pour BMS (membre d'un sous-comité), Janssen (expert urologue), Co-investigateur : Novartis, Janssen-Cilag, Intervention aux JOUM (CCAFU).
Les autres auteurs déclarent ne pas avoir de liens d'intérêts
|
|
|
|
|
| Table 1 - Grade of soft tissue sarcomas according to the FNCLCC: GX (grade cannot be established), G1 (sum of scores: 2-3), G2 (sum of scores: 4-5), G3 (sum of scores 6-7-8). |
| |
Tumour differentiation |
Mitotic Index |
Tumour necrosis |
| Score 0 |
|
|
Absent |
| Score 1 |
Resemblance to normal tissue |
0 to 9 mitoses/10 fields |
Less than 50% |
| Score 2 |
Diagnosis of a definite histological type |
10 to 19 mitoses/10 fields |
More than 5O3/4 |
| Score 3 |
Diagnosis of an uncertain histological type |
> 19 mitoses/10 fields |
|
| Table 2 - TNM 2016 classification of retroperitoneal sarcomas. |
| T - primary tumour (suffix m if multiple primary tumours) |
| Tx |
Cannot be assessed |
| T0 |
No evidence of primary tumour |
| T1 |
Tumour ⤠5 cm in greatest dimension |
| T2 |
Tumour > 5 cm and ⤠10 cm in greatest dimension |
| T3 |
Tumour > 10 cm and ⤠15 cm in greatest dimension |
| T4 |
Tumour > 15 cm in greatest dimension |
| N - Retroperitoneal lymph nodes (suffix sn for sentinel identification or f for cytopuncture/biopsy identification) |
| N0 |
Lymph nodes cannot be assessed |
| N1 |
Lymph node metastases |
| M - Distant metastases |
| cM0 |
No metastasis |
| cM1 |
Distant metastasis |
| pM1 |
Microscopically confirmed presence of distant metastasis |
| Table 3 - AJCC stages according to TNM stage and FNCLCC grade. |
| Stage |
T |
N |
M |
Grade |
| IA |
T1 |
N0 |
M0 |
G1, GX |
| IB |
T2 - T4 |
N0 |
M0 |
G1, GX |
| II |
T1 |
N0 |
M0 |
G2, G3 |
| IIIA |
T2 |
N0 |
M0 |
G2, G3 |
| IIIB |
T3-T4 |
N0 |
M0 |
G2, G3 |
| |
Any stage T |
N1 |
M0 |
Any grade |
| IV |
Any stage T |
Any stage N |
M1 |
Any grade |
| Table 4 - Oncological prognosis according to subtype and histological grade. |
| |
Overall survival at 5 years |
Local recurrence |
Metastatic spread |
| Liposarcoma grade 1 |
87% |
18% |
0% |
| Liposarcoma grade 2 |
54% |
44% |
9% |
| Liposarcoma grade 3 |
41% |
33% |
44% |
| Leiomyosarcoma |
58% |
5% |
55% |
| Tableau 1 - Grade des sarcomes des tissus mous selon la FNCLCC. |
| |
Différenciation tumorale |
Index mitotique |
Nécrose tumorale |
| Score 0 |
|
|
Absente |
| Score 1 |
Ressemblance à un tissu normal |
0 à 9 mitoses/10 champs |
Moins de 50% |
| Score 2 |
Diagnostic de type histologique certain |
10 à 19 mitoses/10 champs |
Plus de 50% |
| Score 3 |
Diagnostic de type histologique incertain |
> 19 mitoses/10 champs |
|
| Tableau 2 - Classification TNM 2016 des sarcomes rétropéritonéaux. |
| T - tumeur primitive (suffixe m si multiples primitifs) |
| Tx |
Non évaluable |
| T0 |
Pas de tumeur primitive identifiée |
| T1 |
Tumeur de grand axe ⤠5 cm |
| T2 |
Tumeur de grand axe > 5 cm et ⤠10 cm |
| T3 |
Tumeur de grand axe > 10 cm et ⤠15 cm |
| T4 |
Tumeur de grand axe > 15 cm |
| N - ganglions rétropéritonéaux (suffixe sn en cas d'identification par sentinelle ou f en cas d'identification par cytoponction/biopsie) |
| N0 |
Pas de ganglion pathologique ou statut inconnu |
| N1 |
Présence de ganglions pathologiques |
| M - métastases à distance |
| cM0 |
Absence de métastase |
| cM1 |
Présence de métastase à distance |
| pM1 |
Présence de métastase à distance confirmée microscopiquement |
| Tableau 3 - Stades AJCC selon le stade TNM et le grade FNCLCC |
| Stade |
T |
N |
M |
Grade |
| IA |
T1 |
N0 |
M0 |
G1, GX |
| IB |
T2 -T4 |
N0 |
M0 |
G1, GX |
| II |
T1 |
N0 |
M0 |
G2, G3 |
| IIIA |
T2 |
N0 |
M0 |
G2, G3 |
| IIIB |
T3 - T4 |
N0 |
M0 |
G2, G3 |
| |
Tout stade T |
N1 |
M0 |
Tout grade |
| IV |
Tout stade T |
Tout stade N |
M1 |
Tout grade |
| Tableau 4 - Pronostic carcinologique en fonction du sous-type et du grade histologique. |
| |
Survie globale à 5 ans |
Récidive locale |
Dissémination métastatique |
| Liposarcome grade 1 |
87 % |
18 % |
0 % |
| Liposarcome grade 2 |
54 % |
44 % |
9 % |
| Liposarcome grade 3 |
41 % |
33 % |
44 % |
| Léiomyosarcome |
58 % |
5 % |
55 % |
| Table recommendation 1 - Treatment recommendations for RPS |
| Treatment recommendations for RPS |
| The therapeutic strategy should be defined from initial care, coordinated by a sarcoma pathology reference centre |
| ± compartmental surgical excision is the cornerstone for treating localised or locally advanced forms of the disease |
| Multimodal, adjuvant or neoadjuvant treatment, by radiotherapy or chemotherapy, optimises the oncological outcomes of high-risk tumours (but does not provide a survival benefit) and should be discussed in a referral MTM |
| Inclusion in therapeutic trials should be offered to patients with RPS in order to define the standards of treatment still under evaluation |
| Overall survival and relapse-free survival are related to the quality of first-line management, including surgical excision, and the volume of cases treated per centre |
| CCAFU |
French Urology Association Cancer Committee |
| CT |
Chemotherapy |
| INCA |
French Cancer Institute |
| MRI |
Magnetic Resonance Imaging |
| PCP |
Personalised Care Program |
| MTM |
Multidisciplinary Team Meeting |
| RT |
Radiotherapy |
| RPS |
Retroperitoneal Sarcoma |
| 18FDG PET |
Positron Emission Tomography |
| Recommandations thérapeutiques pour le SRP |
| La stratégie thérapeutique doit être définie dès la prise en charge initiale, coordonnée par centre de référence en pathologie du sarcome |
| La chirurgie d'exérèse ± compartimentale est la pierre angulaire du traitement des formes localisées ou localement avancées |
| Le traitement multimodal, adjuvant ou néo-adjuvant, par radiothérapie ou chimiothérapie, optimise les résultats carcinologiques des tumeurs à haut risque (sans toutefois apporter de bénéfice en survie) et doit être discuté au sein d'une RCP référente |
| L'inclusion dans des essais thérapeutiques doit être proposée aux patients atteints de SRP afin de définir les standards de traitement encore en évaluation |
| La survie globale et la survie sans récidive sont liées à la qualité de la prise en charge de première intention, notamment de l'exérèse chirurgicale, ainsi qu'au volume de cas traité par centre |
| CCAFU |
Comité de cancérologie de l'Association française d'urologie |
| CT |
Chimiothérapie |
| INCA |
Institut national du cancer |
| IRM |
Imagerie par résonance magnétique |
| PPS |
Programme personnalisé de soins |
| RCP |
Réunion de concertation pluridisciplinaire |
| RT |
Radiothérapie |
| SRP |
Sarcome rétropéritonéal |
| TEP-18FDG |
Tomographie par émission de positons |
|
|
|
|
Renne S.L., Iwenofu O.H. Pathology of retroperitoneal sarcomas: A brief review. J Surg Oncol 2018 ; 117 (1) : 12-24 [cross-ref] |
|
|
|
Dangoor A., Seddon B., Gerrand C., Grimer R., Whelan J., Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res 2016 ; 6 : 20 |
|
|
|
Toulmonde M., Bonvalot S., Méeus P., Stoeckle E., Riou O., Isambert N., et al. Retroperitoneal sarcomas: patterns of care at diagnosis, prognostic factors and focus on main histological subtypes: a multicenter analysis of the French Sarcoma Group. Ann Oncol 2014 ; 25 (3) : 735-742 [cross-ref] |
|
|
|
Cates J.MM. Performance Analysis of the American Joint Committee on Cancer 8th Edition Staging System for Retroperitoneal Sarcoma and Development of a New Staging Algorithm for Sarcoma-Specific Survival. Ann Surg Oncol 2017 ; 24 (13) : 3880-3887 [cross-ref] |
|
|
|
Messiou C., Morosi C. Imaging in retroperitoneal soft tissue sarcoma. J Surg Oncol 2018 ; 117 (1) : 25-32 [cross-ref] |
|
|
|
Roberge D., Vakilian S., Alabed Y.Z., Turcotte R.E., Freeman C.R., Hickeson M. FDG PET/CT in Initial Staging of Adult Soft-Tissue Sarcoma. Sarcoma 2012 ; 2012 : 960194 |
|
|
|
Casali P.G., Abecassis N., Bauer S., Biagini R., Bielack S., Bonvalot S., et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 28 mai 2018 ; 29 : iv51-67 |
|
|
|
Van Houdt W.J., Schrijver A.M., Cohen-Hallaleh R.B., Memos N., Fotiadis N., Smith M.J., et al. Needle tract seeding following core biopsies in retroperitoneal sarcoma. Eur J Surg Oncol 2017 ; 43 (9) : 1740-1745 [cross-ref] |
|
|
|
Fairweather M., Gonzalez R.J., Strauss D., Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol 2018 ; 117 (1) : 33-41 [cross-ref] |
|
|
|
Trans-Atlantic RPS Working Group Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group Ann Surg Oncol 2016 ; 23 (11) : 3531-3540 |
|
|
|
Pham V., Henderson-Jackson E., Doepker M.P., Caracciolo J.T., Gonzalez R.J., Druta M., et al. Practical Issues for Retroperitoneal Sarcoma. Cancer Control 2016 ; 23 (3) : 249-264 [cross-ref] |
|
|
|
Gronchi A., Strauss D.C., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann Surg 2016 ; 263 (5) : 1002-1009 [cross-ref] |
|
|
|
Trojani M., Contesso G., Coindre J.M., Rouesse J., Bui N.B., de Mascarel A., et al. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int J Cancer 1984 ; 33 (1) : 37-42 [cross-ref] |
|
|
|
Amin M.B., Edge S., Greene F., Byrd D.R., Brookland R.K., Washington M.K., et al. AJCC Cancer Staging Manual New York: Springer (2017). |
|
|
|
Pasquali S., Gronchi A. Neoadjuvant chemotherapy in soft tissue sarcomas: latest evidence and clinical implications. Ther Adv Med Oncol 2017 ; 9 (6) : 415-429 [cross-ref] |
|
|
|
Fisher S.B., Chiang Y-J, Feig B.W., Cormier J.N., Hunt K.K., Torres K.E., et al. An Evaluation of the Eighth Edition of the American Joint Committee on Cancer (AJCC) Staging System for Retroperitoneal Sarcomas Using the National Cancer Data Base (NCDB): Does Size Matter?. Am J Clin Oncol 2019 ; 42 (2) : 160-165 [cross-ref] |
|
|
|
Callegaro D., Miceli R., Gladdy R.A. Prognostic models for RPS patients-Attempting to predict patient outcomes. J Surg Oncol 2018 ; 117 (1) : 69-78 [cross-ref] |
|
|
|
Gronchi A., Crago A., Raut C.P. Minimally Invasive Surgery for Retroperitoneal Sarcoma: Just Because We Can Does Not Mean We Should. Ann Surg Oncol 2018 ; 25 (8) : 2129-2131 [cross-ref] |
|
|
|
Bonvalot S., Raut C.P., Pollock R.E., Rutkowski P., Strauss D.C., Hayes A.J., et al. Technical considerations in surgery for retroperitoneal sarcomas: position paper from E-Surge, a master class in sarcoma surgery, and EORTC-STBSG. Ann Surg Oncol 2012 ; 19 (9) : 2981-2991 [cross-ref] |
|
|
|
Fairweather M., Wang J., Jo V.Y., Baldini E.H., Bertagnolli M.M., Raut C.P. Surgical Management of Primary Retroperitoneal Sarcomas: Rationale for Selective Organ Resection. Ann Surg Oncol 2018 ; 25 (1) : 98-106 [cross-ref] |
|
|
|
MacNeill A.J., Gronchi A., Miceli R., Bonvalot S., Swallow C.J., Hohenberger P., et al. Postoperative Morbidity After Radical Resection of Primary Retroperitoneal Sarcoma: A Report From the Transatlantic RPS Working Group. Ann Surg 2018 ; 267 (5) : 959-964 [cross-ref] |
|
|
|
Maurice M.J., Yih J.M., Ammori J.B., Abouassaly R. Predictors of surgical quality for retroperitoneal sarcoma: Volume matters. J Surg Oncol 2017 ; 116 (6) : 766-774 [cross-ref] |
|
|
|
Ikoma N., Roland C.L., Torres K.E., Chiang Y.J., Wang W.L., Somaiah N., et al. Concomitant organ resection does not improve outcomes in primary retroperitoneal well-differentiated liposarcoma: A retrospective cohort study at a major sarcoma center. J Surg Oncol 2018 ; 117 (6) : 1188-1194 [cross-ref] |
|
|
|
Bonvalot S., Gaignard E., Stoeckle E., Meeus P., Decanter G., Carrere S., et al. Survival Benefit of the Surgical Management of Retroperitoneal Sarcoma in a Reference Center: A Nationwide Study of the French Sarcoma Group from the NetSarc Database. Ann Surg Oncol 2019 ; 26 (7) : 2286-2293 [cross-ref] |
|
|
|
Zerhouni S., Van Coevorden F., Swallow C.J. The role and outcomes of palliative surgery for retroperitoneal sarcoma. J Surg Oncol 2018 ; 117 (1) : 105-110 [cross-ref] |
|
|
|
Haas R.L., Baldini E.H., Chung P.W., van Coevorden F., DeLaney T.F. Radiation therapy in retroperitoneal sarcoma management. J Surg Oncol 2018 ; 117 (1) : 93-98 [cross-ref] |
|
|
|
Diamantis A., Baloyiannis I., Magouliotis D.E., Tolia M., Symeonidis D., Bompou E., et al. Perioperative radiotherapy versus surgery alone for retroperitoneal sarcomas: a systematic review and meta-analysis. Radiol Oncol 2020 ; 54 (1) : 14-21 [cross-ref] |
|
|
|
Haas R.LM., Bonvalot S., Miceli R., Strauss D.C., Swallow C.J., Hohenberger P., et al. Radiotherapy for retroperitoneal liposarcoma: A report from the Transatlantic Retroperitoneal Sarcoma Working Group. Cancer 2019 ; 125 (8) : 1290-1300 [cross-ref] |
|
|
|
Bates J.E., Dhakal S., Mazloom A., Constine L.S. The Benefit of Adjuvant Radiotherapy in High-grade Nonmetastatic Retroperitoneal Soft Tissue Sarcoma: A SEER Analysis. Am J Clin Oncol 2018 ; 41 (3) : 274-279 |
|
|
|
Almond L.M., Gronchi A., Strauss D., Jafri M., Ford S., Desai A. Neoadjuvant and adjuvant strategies in retroperitoneal sarcoma. Eur J Surg Oncol 2018 ; 44 (5) : 571-579 [cross-ref] |
|
|
|
Naghavi A.O., Fernandez D.C., Mesko N., Juloori A., Martinez A., Scott J.G., et al. American Brachytherapy Society consensus statement for soft tissue sarcoma brachytherapy. Brachytherapy 2017 ; 16 (3) : 466-489 [cross-ref] |
|
|
|
Miura J.T., Charlson J., Gamblin T.C., Eastwood D., Banerjee A., Johnston F.M., et al. Impact of chemotherapy on survival in surgically resected retroperitoneal sarcoma. Eur J Surg Oncol 2015 ; 41 (10) : 1386-1392 [cross-ref] |
|
|
|
Italiano A., Delva F., Mathoulin-Pelissier S., Le Cesne A., Bonvalot S., Terrier P., et al. Effect of adjuvant chemotherapy on survival in FNCLCC grade 3 soft tissue sarcomas: a multivariate analysis of the French Sarcoma Group Database. Ann Oncol 2010 ; 21 (12) : 2436-2441 [cross-ref] |
|
|
|
Datta J., Ecker B.L., Neuwirth M.G., Geha R.C., Fraker D.L., Roses R.E., et al. Contemporary reappraisal of the efficacy of adjuvant chemotherapy in resected retroperitoneal sarcoma: Evidence from a nationwide clinical oncology database and review of the literature. Surg Oncol 2017 ; 26 (2) : 117-124 [cross-ref] |
|
|
|
Bonvalot S., Cavalcanti A., Le Péchoux C., Terrier P., Vanel D., Blay J.Y., et al. Randomized trial of cytoreduction followed by intraperitoneal chemotherapy versus cytoreduction alone in patients with peritoneal Sarcomatosis. Eur J Surg Oncol 2005 ; 31 (8) : 917-923 [cross-ref] |
|
|
|
Tan M.CB., Brennan M.F., Kuk D., Agaram N.P., Antonescu C.R., Qin L.X., et al. Histology-based Classification Predicts Pattern of Recurrence and Improves Risk Stratification in Primary Retroperitoneal Sarcoma. Ann Surg 2016 ; 263 (3) : 593-600 [cross-ref] |
|
|
|
Avancès C., Mottet N., Mahatmat A., Chapuis E., Serre I., Culine S. Prognostic factors for first recurrence in patients with retroperitoneal sarcoma. Urol Oncol 2006 ; 24 (2) : 94-96 |
|
|
|
Gronchi A., Miceli R., Shurell E., Eilber F.C., Eilber F.R., Anaya D.A., et al. Outcome prediction in primary resected retroperitoneal soft tissue sarcoma: histology-specific overall survival and disease-free survival nomograms built on major sarcoma center data sets. J Clin Oncol 2013 ; 31 (13) : 1649-1655 [cross-ref] |
|
|
|
Gronchi A., Miceli R., Allard M.A., Callegaro D., Le Péchoux C., Fiore M., et al. Personalizing the approach to retroperitoneal soft tissue sarcoma: histology-specific patterns of failure and postrelapse outcome after primary extended resection. Ann Surg Oncol 2015 ; 22 (5) : 1447-1454 [cross-ref] |
|
|
|
Zaidi M.Y., Canter R., Cardona K. Post-operative surveillance in retroperitoneal soft tissue sarcoma: The importance of tumor histology in guiding strategy. J Surg Oncol 2018 ; 117 (1) : 99-104 [cross-ref] |
|
|
|
MacNeill A.J., Miceli R., Strauss D.C., Bonvalot S., Hohenberger P., Van Coevorden F., et al. Post-relapse outcomes after primary extended resection of retroperitoneal sarcoma: A report from the Trans-Atlantic RPS Working Group. Cancer 2017 ; 123 (11) : 1971-1978 [cross-ref] |
|
|
|
|
|
|
|
© 2020 Elsevier Masson SAS. Tous droits réservés. |
|
|
|
|
|