Kidney cancer is the 6th most common cancer. In France, there were 15,323 new cases of kidney cancer in 2018 with an increase in incidence of 1.7% per year in men and 1.4% in women between 1990 and 2018. In 2018, kidney cancer was responsible for 5,589 deaths in France, i.e. a mortality rate of 5 and 1.5 deaths per 100,000 inhabitants in men and women respectively [1]. Age and gender are two non-modifiable risk factors, with a male to female gender ratio of 1.5 and peak incidence between 60 and 70 years of age [1]. The two main modifiable risk factors for kidney cancer are smoking and obesity [1, 2]. High blood pressure has also been identified as a potential risk factor for kidney cancer and control of blood pressure in hypertensive patients could be beneficial [3]. Physical activity could reduce the risk of kidney cancer, notably by reducing obesity and high blood pressure [4]. Patients with chronic renal failure have an increased risk of developing kidney cancer (up to ten times higher than the general population), with frequent bilateral and/or multiple site involvement [5, 6]. The CCAFU recommendations for prevention are shown in #tabr1.
|
|
Diagnostic evaluation of renal tumours |
|
| Imaging techniques: technique and results |
Diagnosis and characterization of renal masses are based on three complementary imaging techniques, Doppler ultrasound, CT scan and MRI, which can be performed with or without the injection of contrast medium.
Renal tumours are often often diagnosed by this imaging modality. It provides the basic information concerning characteristics of the tumour: cystic or solid tumour, typical or atypical, markedly hyperechoic in nature and suggestive of angiomyolipoma (AML). Along with the Doppler, it evaluates tumour vascularisation and can be useful in vascular staging (renal vein, inferior vena cava). It can be usedin active surveillance to measure renal tumour diameter. Finally, it enables effective guidance of biopsy when applicable through a real time image of the needle path.
Intravenous injection of a contrast medium (Sonovue®) improves the characterisation of poorly vascularised solid tumours, atypical cystic tumours and venous thrombus (tumour vs. cruor), and guidance of the biopsy to non-necrotic areas in case of large tumours [7, 8, 9]. In clinical practice, tolerance to this contrast medium is excellent, and there are no contraindications related to renal function [7].
In practice, the place of Doppler ultrasound is limited to preoperative evaluation of renal tumours.
|
|
Computed tomography (CT scan) |
|
|
Iodinated contrast media (ICM) |
ICM are the least tolerated contrast media, and the incidence of hypersensitivity reactions is up to 3%, including 0.04% of severe anaphylactic reactions, and a risk of decline in renal function ranging from 2 to 6% depending on the route of administration for low osmolality contrast media [10, 11, 12]. Patients at risk for induced nephropathy are those with 1) acute renal failure, 2) a glomerular filtration rate (GFR) of less than 45 ml/min/1.73 m2 for suprarenal intra-arterial injection or being hospitalised in intensive care, 3) or GFR of less than 30 ml/min/1.73 m2 for subrenal intra-arterial injection or intravenous injection (e.g. CT scan). In patients at risk, either an alternative imaging modality (MRI/ultrasound with injection) should be offered or hyperhydration should be ensured, with ICM injections spaced at least 3 days apart, the injected dose limited to the minimum that is necessary, and creatinine levels monitored 48 to 72 hours after injection.
Haemodialysis after contrast injection does not reduce the renal toxicity of ICM [12]. However, in patients on dialysis, it is preferable to perform a CT scan with injection rather than an MRI with injection if the diagnostic benefit is equivalent. In diabetic patients treated with metformin, there is no need to discontinue therapy due to the risk of lactic acidosis if the GFR is above 30 ml/min/1.73 m2. When the GFR is less than 30 ml/min/1.73 m2, metformin should be discontinued on the day of the injection until creatinine levels are checked in 48 hours. It can only be restarted if there is no significant change in renal function. Finally, depending on renal function, myeloma is no longer an absolute contraindication for ICM injection, even secretory and light chain types [13].
CT scan is the gold standard for the evaluation of renal tumours in the absence of ICM contraindications. The dose of ICM should be sufficient to enable detection of the enhancement of hypovascular tumours and Bosniak III and IV cystic masses (0.2 ml/kg of a medium containing iodine 350 mg/ml). CT scan should include the following four phases:
• | An acquisition without injection which is essential to define the contrast (> + 20 HU between the tubular phase and the acquisition without injection).
|
• | An acquisition at the cortical nephrography phase, 30 to 40 seconds after injection.
|
• | An acquisition at the tubular nephrography phase 80 to 100 seconds after injection (different from the portal phase acquired 60 seconds after injection on which the medulla is not yet enhanced).
|
• | A late excretory acquisition.
|
These phases can be combined, according to the indications, in order to limit irradiation. The acquisition at the excretory phase depends on the indication (identification of late enhancement, examination of the relationship of the tumour with the urinary tract) [14, 15, 16]. For renal imaging, patients should not be fasting and the gastrointestinal tract should not be opacified.
Dual-energy spectral CT is a new technology with promising results for the evaluation of renal pthologies [17]. With the introduction of new multilayer sensors and high-speed reconstructors, it could provide access to mono-energetic images and iodine mapping in standard practice. These examinations, which are less irradiating, could be performed with an ICM volume of less than 50 ml. It limits the artefacts related to the pseudoenhancement of central renal masses and metal artefacts and could improve the characterization of renal tumours, as, among other things, it is more sensitive to the enhancement of poorly vascularised masses (papillary carcinomas) [18, 19, 20].
CT scan is the method of choice to identify AML because it can detect macroscopic fat islets (density < -20 HU). Uncommonly, there might be fat metaplasia associated with calcifications in clear cell carcinomas. Macroscopic fat-free AMLs may have moderate spontaneous hyperdensity (density > 45 HU) and homogeneous enhancement [21].
Cystic lesions should be analysed according to the Bosniak classification, which distinguishes five categories according to the risk of malignancy. This classification applies to cystic masses excluding any infectious context or autosomal dominant polycystic disease. Nevertheless, there is significant variability in malignancy rates related to diagnostic criteria, study biases, acquisition technique and imaging method (CT scan vs. MRI vs. contrast ultrasound).
CT scan also provides elements of tumour characterization for renal carcinoma types, according to whether the enhancement is hypervascular or homogeneous. Nevertheless, these elements are only indicative and should prompt the performance of a renal biopsy if the results can impact further management.
CT scan with contrast injection is the key examination in the preoperative evaluation of renal tumours. Whenever possible, it should include a pre-injection examination and three post-injection phases, with multiplanar and MIP reconstructions. It allows precise evaluation of the tumour (size, location, relationship to the upper urinary tract and vessels) and perirenal fat. Classification according to RENAL or PADUA scores may be useful in predicting the complexity of partial nephrectomy [22]. It helps in locoregional (veins, lymph nodes, adrenal glands) and metastatic (lung, liver, pancreas) staging and in case of vena cava thrombosis should specify the level of the upper portion of the thrombus in relation to the diaphragm and the ostium of the suprahepatic veins. It identifies synchronous tumours in the contralateral kidney.
MRI has become more than a substitute modality for CT scan in case of contraindications to ICM injection (renal failure with GFR < 30 ml/min, history of anaphylactic reaction to ICM injection). It is indicated for the characterization of cystic and atypical solid masses that have remained undetermined on CT scan, for staging (particularly vascular), and to monitor patients with hereditary cancer. However, the pre-therapeutic evaluation of renal tumours is still primarily based on a CT scan.
|
|
Gadolinium-based contrast agents (GBCA) [11, 12] |
They are very well tolerated in clinical practice and nephrogenic systemic fibrosis is now a very exceptional side effect, if not non-existent. It used to occur in patients with acute renal failure (GFR < 15 ml/min/1,73 m2) or who were on dialysis, and the incidence was related to the stability of the chelate complex Gadolinium. In at-risk patients, injection is currently not contraindicated if the clinical benefit outweighs the risk, which is the case with kidney cancer, but only products with high stability should be used (Gadobutrol, Gadoterate meglumine and Gadoteridol). GBCAs can lead to an accumulation of Gadolinium in the basal ganglia but, to date, there is no specific neurological symptomatology related to these deposits. There are also deposits in bone, liver (asymptomatic) and skin, which cause erythematous plaques similar to those in nephrogenic systemic fibrosis (but in the absence of renal failure).
The multiparametric examination comprises axial and coronal T2-weighted sequences with and without fat signal saturation, T1-weighted gradient echo in-phase and opposed-phase sequences (detection of intra-tumour fat on the opposed-phase sequence), high b-value diffusion (800 to 1,000), and finally a dynamic sequence after contrast injection with late acquisition (tumour washout study, contrast acquisition of the stellate central fibrotic scar of oncocytoma).
The T2-weighted sequences (with or without fat signal saturation) make it possible to distinguish solid tumours from typical (even infracentimetric) or atypical cystic lesions, and to a lesser extent AML (even low-fat) in T2 hyposignal (haemorrhagic suffusions, papillary formations or muscle cells) [23, 24]. Clear cell carcinomas and oncocytic tumours often have a hypersignal [25, 26]. The dynamic T1 -weighted sequence before and after injection of GBCA distinguishes hypervascular and heterogeneous tumours (corresponding to clear cell carcinomas and AMLs) from homogeneous less enhanced (chromophobe carcinomas) or poorly enhanced (papillary carcinomas) tumours. The presence of a signal drop in the opposed-phase and on fat saturation sequences is not specific for a low fat component AML, as it is present for many carcinomas [27]. MRI can also be used to identify microcystic territories or necrotic haemorrhagic changes. A hypovascular stellar central area is consistent with the diagnosis of oncocytoma but can also be found in renal carcinomas [28]. Diffusion imaging is very sensitive to detect small infracentimetric tumours that are difficult to characterize by other sequences and during staging or surveillance to identify lymph node, adrenal, pancreatic or liver metastases.
While MRI provides guidance for identifying the different types of solid tumours, itdoes not allow a histological diagnosis to be made with certainty due to the lack of specificity of the different signs combined. Biopsy remains essential when the subsequent therapeutic course can be modified by the histological results [29].
Fluorine-18-fluorodeoxyglucose (F-FDG) PET CT is used to stage many cancers. It is not useful in the characterization of renal tumours. On the other hand, it could be useful at the time of staging or after surgery to detect recurrences. A recent meta-analysis evaluated its sensitivity at 0.86 (95% CI, 0.88–0.93) and specificity at 0.88 (95% CI, 0.84– 0.91) in detecting metastases. However, further prospective studies are needed to define its place and the additional information it could provide compared to the conventional CT scan [30].
Standard staging is based on thoracic and abdominal CT scan with and without injection, and the thoraco-abdomino-pelvic scan should be performed at the time of arterial nephrography. If there is a strict contraindication to the injection of an ICM, a thoraco-abdominal CT scan without injection can be combined with an abdominal MRI with and without injection.
|
| Anatomical classifications |
Different morphometric classifications have been reported with the aim of assisting the clinician with surgical planning and informing the patient in preparation for conservative surgery [31]. The oldest are the RENAL [22] and PADUA [32] scores but over the past 10 years, 16 other classifications have been presented [33]. The vast majority of available studies are retrospective. The predictive values of the RENAL and PADUA scores are higher when they are used as categorical variables and in particular for estimating the risk of global or major perioperative complications and the duration of renal ischaemia. Their major interest is to provide objective categorisation of tumour characteristics allowing comparability with the scientific literature.
The modalities and indications for imaging examinations are summarized in #tabr2.
|
|
Standard biological examination |
The standard biology examination for renal tumour should include:
• | Serum creatinine test,
|
• | Blood count.
|
In case of metastatic cancer, the following should be added:
• | LFTs,
|
• | Alkaline phosphatases,
|
• | LDH,
|
• | Serum calcium with corrected serum calcium,
|
• | Coagulation assessment.
|
The aim is to evaluate renal function, determine prognostic factors (for metastatic tumour) and to screen for a possible paraneoplastic syndrome: anaemia, polycythaemia, hypercalcaemia, cholestasis [34, 35].
|
|
Kidney function assessment |
The reference technique for estimating glomerular filtration rate is the calculation of creatinine clearance according to the Chronic Kidney Disease Epidemiology Collaboration 2009 (CKD EPI) equation. The CKD EPI equation is considered to be more effective than the Cockroft/Gault and MDRD (Modification of Diet in Renal Disease) methods [36]. However, there are situations in which the calculation of creatinine clearance does not provide a reliable assessment of renal function: extreme situations concerning muscle mass (obesity, cachexia), inhibition of renal tubular secretion (trimethoprim and fenofibrate) and extra-renal creatinine elimination by microbiota (broad-spectrum antibiotic therapy) [36]. It is advisable to evaluate renal function separated by scintigraphy in case of renal failure or bilateral tumours [37].
|
| What elements should be displayed in a standard pathology report? |
The pathology report is a key element in the prognostic assessment and management of patients. The French Pathology Society and the French Cancer Institute have developed standardised reports with items that must appear in each conclusion for kidney cancer (French Pathology Society http://www.sfpathol.org/; French Cancer Institute www.e-cancer.fr.).
A typical conclusion for kidney cancer should include a number of items that are listed in Table 1 [1, 2].
|
| Main histological subtypes |
There has been no change in histological subtypes since the last WHO 2016 classification of urological and male genital tract tumours [3, 4]. However, many entities are still in the process of being categorised, particularly oncocytic renal tumours and renal carcinomas with a leiomyomatous stroma (Table 2).
Unclassified renal cell carcinomas (approximately 6% of renal malignancies), with a metastatic risk, are defined as follows: 1) tumour does not meet the diagnostic criteria for the classic histological subtypes of renal cell carcinomas or 2) unclassified low-grade oncocytic carcinoma or 3) tumour with a pure sarcomatoid component [5].
Other renal tumours are much rarer and are of haematopoietic, mesenchymal, metanephric, nephroblastic, endocrine, germinal or metastatic origin.
It is recommended to use the 2017 classification reviewed in 2019 by the American Joint Committee on Cancer /AJCC which is identical to the Union for International Cancer Control/ UICC 2017 pTNM classification (Table 3) [6, 7, 8]. Compared to the previous 2010 pTNM classification, infiltration of pyelocalicial cavities has been added in the pT3a stage.
Several emerging entities are still in the process of being categorised, including oncocytic tumours. Among these tumours, oncocytomas and chromophobe oncocytic carcinomas are well known to uropathologists and have a common feature of membrane positivity in CD117 immunohistochemistry. CK7 is negative or sparse in oncocytomas, whereas it is strong and diffused in chromophobe carcinomas, although it may be negative in 30% of the cases [9].
Recently, the following emerging entities have been reported [10, 11, 12]:
• | Low-grade oncocytic tumours (LOT): this is a renal tumour with oncocytic cells that often have a solid architecture, but which has the particularity of being CD117-negative and CK7-strongly positive. Few cases have been described but progression seems to be benign.
|
• | High-grade oncocytic tumours (HOT) are renal tumours that also have oncocytic cells, often with a solid architecture and the same immunohistochemical profile as oncocytoma with CD117 positivity, and CK-negative or focally positive. This tumour has the particularity of presenting very prominent nucleoli, hence the use of the term high-grade, whereas in principle, they are nonaggressive small tumours.
|
|
| Oncogenetics: in which cases? |
Hereditary predispositions to renal tumours occur in approximately 5% of the adult cases. There are 11 syndromes with 17 identified genes: VHL, MET, FH, SDHA, SDHB, SDHC, SDHD, PTEN, BAP1, PBRM1, TSC1, TSC2, FLCN, MITF, CDC73, CDKN2B and HNF1β. The incidence of these hereditary predispositions is higher in non-clear cell carcinomas (12% versus 3% for clear cell carcinomas).
The renal tumours most frequently encountered in these predispositions are clear cell, papillary, chromophobe cell carcinomas and angiomyolipomas.
The most common hereditary syndromes are listed in Table 4.
The criteria for suggesting oncogenetic consultation are listed in Table 5.
Biopsy can be performed under local anaesthesia as an outpatient procedure with ultrasound or CT guidance. The CCAFU recommends the use of a 16–18 G coaxial needle to prevent the risk of tumour dissemination, to avoid targeting necrotic areas and to harvest at least two samples.
The diagnostic performance of the biopsy is best when:
• | The tumour is solid rather than cystic.
|
• | A biopsy needle is used rather than fine needle aspiration [ 38]. |
Cytoponction is not effective and is no longer recommended [38].
Biopsies should be fixed in 4% buffered formaldehyde which allows histological analysis, FISH and genetic sequencing. Unfixed conditioning for freezing is recommended for paediatric renal tumours, but freezing is optional for adult renal tumours.
|
| Diagnostic performance and complications |
In centres with a high level of expertise, biopsy performs well in establishing the diagnosis of malignancy, but there are frequent cases of non-contributive biopsies (absence of tumour tissue or histological material not sufficient for a proper histologic evaluation).
In 2016 two systematic reviews of the literature evaluated the performance of renal biopsy [38, 39]:
• | For the diagnosis of malignancy, sensitivity and specificity were > 95%.
|
• | For the determination of the histological subtype, the biopsy/surgical specimen concordance was 90%.
|
• | The diagnosis of oncocytoma is difficult on biopsy: it can be challenging to distinguish from chromophobe carcinoma and 25% of patients have a final diagnosis of clear cell carcinoma [ 39]. |
• | For nuclear grading, the performance of kidney biopsy ranged from 43% to 93%. For renal tumours of < 4 cm, grade concordance was 86% with a simplified high/low grade classification. In the majority of cases, the grade error consisted of an underestimation compared to the surgical specimen [ 40, 41]. |
• | Major complications were rare (2%) [ 38]. |
• | Biopsy needle track seeding was exceptional [ 42]. |
• | The rate of non-contributivebiopsies could be as high as 20%.
|
The performance of biopsy varies greatly in France and it is difficult to specifically delineate the indications. There are more and more questions concerning the « medico-legal » aspect of biopsy which could prevent surgery of of benign tumour.
The CCAFU recommends a biopsy for renal tumours when the histological diagnosis is likely to impact further management. It is also recommended to inform the patient about the possibility of performing a biopsy, and its capacities and limitations. Table 6 summarises the indications for which biopsies are recommended or not. Levels of evidence and recommendations are indicated in #tabr3.
|
| The place of biopsy in small tumours |
For tumours < 4 cm, the diagnostic contribution of the biopsy is 90% [41,43]. Sensitivity and specificity for the diagnosis of malignancy are > 95%. The concordance for the histological subtype is 96% and for the grade 87% [44].
Recently, several studies have suggested that biopsy may change the management of small renal masses, particularly by reducing the rate of interventions for benign tumours [40].
Concerning oncocytomas, several series have reported reassuring results concerning the surveillance strategy after biopsy confirmation [45, 46, 47, 48, 49, 50]. Oncocytomas grow slowly (0.1 to 0.5 cm/year), but the negative predictive value of biopsy is not excellent, with histological correlations between biopsy and surgical specimen ranging from 65% to 100%.
|
|
Treatment of small renal tumours T1a (< 4 cm) |
|
| The place of partial nephrectomy (PN) |
PN is the standard technique for small renal masses. It should meet three requirements: oncological control, preservation of renal function and limitation of perioperative complications.
PN provides oncological control identical to RN [51]. After PN for T1a tumour, the 5-year relapse-free survival is > 95% [51].
A positive surgical margin increases the risk of local recurrence but does not seem to have any impact on disease-specific survival [52, 53, 55]. In case of a positive surgical margin, simple surveillance by regular imaging examinations is recommended. Immediate total nephrectomy is not necessary [53,55]. In case of an aggressive tumour of high grade and/or with large positive margin, RN can be discussed in the MTM.
The treatment of local recurrence has been poorly evaluated. RN, a second PN or ablation therapy can be decided depending on the time to recurrence, histological type, and grade [55].
|
|
Preservation of renal function |
PN allows optimal preservation of the renal parenchyma, which limits the deterioration of renal function [56]. This functional preservation reduces the risk of cardiovascular events and may increase overall survival compared to RN [57, 58, 59, 60]. Kidney preservation is also associated with a positive psychological impact and improvement in quality of life (61).
Duration of ischaemia - The impact of the duration of ischaemia on the decline in renal function is discussed matter of debate. Renal ischaemia may have a more detrimental effect in patients with pre-existing renal insufficiency [60]. The data in the literature is contradictory, but it is advisable to limit the period of clamping of the renal pedicle to less than 25 min [62]. Non-clamping or selective clamping techniques have not been shown to provide better renal preservation than total clamping < 25 minutes [63, 64].
Preservation of parenchymal volume - Preservation of healthy kidney parenchyma appears to be the most important factor in maintaining kidney function [62,65]. Tumour enucleation techniques that preserve a minimal margin of healthy tissue do not appear to increase the rate of local recurrence, but their contribution to preserving renal function is uncertain [10,66,67].
PN is associated with a significant morbidity, which is approximately 20% according to the literature. The two most feared complications are secondary bleeding (false aneurysm) and urinary fistula. The rate of serious complications after PN can be as high as 11%. The risk of complications is influenced by many factors: tumour complexity, age, co-morbidities, the surgeon’s experience, the volume of the centre, the type of surgical approach [68, 69].
|
|
Technique: open vs. laparoscopic vs. robot-assisted laparoscopic approach |
Regardless of PN approach (open vs. laparoscopic vs. robotic-assisted), there is no difference in terms of disease-specific survival and overall survival [70, 71].
Compared to the open approach, laparoscopy reduces blood loss and length of stay. Conversely, the operating and ischaemia times are longer. Postoperative complications and long-term renal function are similar [70, 71]. This is a technically difficult approach that is hardly used any more. Some teams propose preoperative tumour embolisation to facilitate the surgical procedure and reduce postoperative complications, but this is a technique that is still under development and its dissemination remains modest [73].
Compared to the open approach, robot-assisted laparoscopy has an advantage in terms of blood loss, length of stay, complications and the duration of ischaemia. The rate of positive margins and residual renal function are similar [71,74, 75].
Compared to the laparoscopic approach, the robotassisted approach has an advantage in terms of the duration of ischaemia, conversion to the open approach, changes in glomerular filtration rate and length of stay [76]. There is also a benefit in terms of the rate of conversion to RN, especially for complex and hilar tumours [71,76, 77]
|
|
The centre effect in France |
A 2010 prospective study conducted at French university and private hospital facilities suggested a centre effect of PN with an increase in morbidity and the rate of positive margins in smaller centres [78]. A more recent CCAFU study also showed better results for robot-assisted PN in larger centres [25,79]. While it is difficult to make recommendations on a possible threshold, the CCAFU encourages teams to organise themselves so that PN is performed only by a few expert surgeons according to the volume of activity.
Levels of evidence and recommendations concerning the indications for PN in T1a tumours are provided in #tabr4.
|
| The place of radical nephrectomy (RN) |
RN is not recommended as a first-line treatment for small renal tumours. It may be offered in case of a non-functioning kidney, suspicion of a T3a tumour or significant complexity. If a tumour is considered to be too complex, it is recommended to refer the patient toan expert centre before deciding to perform a RN.
|
|
Technique: open vs. laparoscopic vs. robot-assisted laparoscopic approach |
The oncological outcomes of the different approaches are equivalent [80]. Laparoscopy is associated with a shorter hospital stay, a reduction in the use of analgesics and a reduction in intraoperative bleeding [81]. Trans- and retroperitoneal laparoscopic approaches have equivalent oncological and quality of life outcomes [82]. Very few studies compared the robot-assisted technique with standard laparoscopy, for which the results seem to be equivalent [83].
|
| The place of ablation therapy |
Small renal tumours can be treated by ablation therapy (AT). A preliminary diagnostic biopsy is recommended. There are different AT techniques:
• | Radiofrequency and microwaves,
|
• | Cryotherapy.
|
• | Recently, irreversible electroporation or stereotactic radiotherapy.
|
The indications for AT are summarised in Table 7
AT can be considered as an option for patients with tumours that can be fully treated. The long-term technical and functional results of AT are good [51,84,85]. There are no randomised studies that compare AT to PN and published retrospective studies have many biases. However, local oncological control after AT appears to be lower than with PN [5184, 85, 86, 87]. Some retrospective studies suggest better preservation of renal function in comparison to PN [88, 89]. The rate of overall and major complications appears to be lower for AT than for PN [39,92, 93].
Comparison of AT to PN - There are no randomised studies that compare the two techniques. All the recommendations are based on retrospective studies. A recent meta-analysis of 26 studies and 11 systematic reviews was published by the EAU Renal Cell Cancer Guidelines Panel. The conclusion was that the level of evidence was very low for AT and that it was difficult in this context to make recommendations in comparison to PN. The CCAFU recommends that patients be informed that AT provides good oncology outcomes even if they are inferior to those provided by PN, but that long-term data is uncertain.
|
| The place of active surveillance |
Active surveillance (AS) is defined as the regular monitoring of the size of a renal tumour by repeated imaging examinations (ultrasound, CT scan or MRI). Treatment may be offered if the tumour increases in size [94].
Biopsy is not a systematically required for AS.
The indications are:
• | Elderly patients.
|
• | Patients with significant co-morbidities.
|
• | Small renal tumours < 4 cm [ 265]. |
There are no randomised trials of AS in patients with small renal masses. However, several prospective registry studies are available [95, 96].
The DISSRM’s main multicentre registry studied the feasibility of AS for tumours < 4 cm and reported similar overall (92 vs. 75%; p = 0.06) and disease-specific (99% vs 100%; p = 0.3) survival at 5 years between patients treated immediately (with PN or AT) and those who were initially monitored [97]. The update of this data at 7 years confirmed the feasibility of AS, reporting similar disease-specific survival between PN and AS [98]. However, a non-controlled prospective study by MD Anderson reported a decrease in overall survival at 2 years for surveillance (versus surgery) for tumours larger than 3 cm, suggesting a 3 cm threshold for AS [99].
In terms of quality of life, compared to patients who had a procedure immediately (surgery or ablation therapy), patients on AS were in poorer physical health (but they were older patients with co-morbidities) and showed more anxiety [100, 101].
Surveillance is possible for T1b tumours, even though only very fragmented data is available. It is reserved for elderly and inoperable patients [102].
Levels of evidence and indications for AS and AT for small renal tumours are provided in #tabr5.
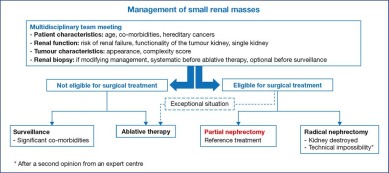
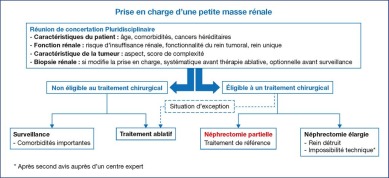
The management of a small renal mass is summarized in Figure 1.
Figure 1.
Algotithm for the management of a small renal tumour.
|
|
Treatment of localised renal tumours > 4 cm |
|
| The place of partial nephrectomy |
PN and RN have identical oncological outcomes for tumours > 4 cm. PN improves the preservation of renal function but seems to be associated with higher perioperative morbidity [103, 104, 105].
The complexity of the tumour can be assessed by morphometric scores (RENAL score, PADUA score, C-Index). These scores could be of interest to predict alteration ofrenal function and prognosis in case of tumours > 7 cm [106, 107, 108]. An increase in tumour size and complexity is associated with an increase in the risk of pT3a tumour and local recurrence [107,109, 110].
The robot-assisted laparoscopic approach appears to decrease the morbidity of PN for tumours > 4 cm. It is associated with less bleeding, fewer complications and a shorter hospital stay than open surgery [111, 112]. The associated intraoperative morbidity is comparable to that of RN [113].
Therefore, PN should be prioritized in T1b tumours whenever technically feasible.
|
| The place of radical nephrectomy |
RN is indicated when PN is not technically feasible (tumour complexity, tumour too large, insufficient surgical expertise) or when the kidney is no longer functional.
It is not necessary to perform an adrenalectomy unless adjacent tissue involvement is detected during surgery or an abnormality suggestive of a secondary lesion is noted on the preoperative imaging [114, 115].
Lymphadenectomy is not recommended for cN0 patients. While some retrospective studies have suggested a possible survival benefit, a randomised study by the EORTC showed no benefit [116, 117].
In terms of surgical technique, no difference was reported in oncologic control between laparoscopic RN and open SN. Laparoscopy reduces blood loss, postoperative pain, length of hospital stay and convalescence [118]. Robot-assisted laparoscopy has oncological and functional outcomes that are comparable to standard laparoscopy [119, 120]. No oncological difference was found between the retroperitoneal and the trans-peritoneal approach [121, 122].
|
| The place of thermal ablation |
Few studies have reported the results of TA for tumours larger than 4 cm and length of follow-up are short [123, 124]. The data is insufficient to recommend their use in this indication.
Treatment recommendations for cT1-2 N0 M0 tumours are shown in #tabr6.
|
|
Treatment of locally advanced kidney cancer |
|
| Definition of locally advanced kidney cancer |
Locally advanced kidney cancers are those that are neither intracapsular (pT1, pT2) nor metastatic (M1).
|
| Principles of radical nephrectomy |
|
|
Technique: open vs. laparoscopic and robotassisted laparoscopic |
In this case, surgery has a curative intent. The main objective with any technique is to achieve negative surgical margins [125]. The standard approach for locally advanced renal tumours is the open approach. Several series have reported the feasibility of the laparoscopic or robot-assisted laparoscopic approach, which can be used provided that macroscopicnegative margins can be obtained [126, 127, 128].
|
|
Value and indications for lymphadenectomy |
Lymphadenectomy is recommended in case of macroscopic adenopathies identified on preoperative imaging or during surgery [129]. Surgical excision of identified adenopathies in a non-metastatic patient could be of prognostic as well as therapeutic interest (oligometastasis) [130, 131].
In the absence of identified adenopathy, the oncological value of lymph node dissection has not been demonstrated, with a rate of positive lymph nodes from lymphadenectomy ranging from 3% to 21% [4,7, 8-9]. If lymph node involvement is proven, the survival rate after nephrectomy is 10% to 45% at 5 years [134].
|
| The role of adjuvant and neoadjuvant therapies |
Patients with locally advanced tumours have a high risk of metastatic progression. It is recognized that after surgery, 30% to 40% of patients will progress to metastatic disease [135].
Most randomised studies that have investigated the value of adjuvant anti-angiogenic therapy in patients at high risk for relapse after nephrectomy have reported negative results (Table 8) [138]. Only the S-Trac study, which evaluated the benefit of treatment with sunitinib in patients at high risk for relapse, demonstrated an increase in disease-free survival but no benefit in overall survival in the sunitinib group [139]. Adjuvant therapy may increase overall survival in the high-risk patient population, but there is no consensus on the definition of this population [140, 141]. Many studies are under way that examine the value of adjuvant immunotherapy in cancers with a high risk of recurrence after surgery [142].
A systematic review of the literature that examined the value of adjuvant radiotherapy found that it was associated with a decrease in the risk of local recurrence, but without any impact on overall or disease-specific survival [143].
Neoadjuvant use of targeted therapies provides a limited response to the primary tumour (9–28%) and this therapeutic strategy is not recommended [144, 145, 146]. The place of neoadjuvant immunotherapies is being evaluated and they should only be used in clinical trials or discussed in MTM on a case-by-case basis [147]. They should be considered with caution as they may be associated with increased surgical difficulties associated with peritumoral inflammatory changes following immunotherapy [148].
|
|
Invasion of adjacent organs |
Invasion of adjacent organs is difficult to predict [149]. Many cT4 patients are over-staged and may benefit from surgical resection. Survival at this stage is less than 10% at 5 years, and the existence of negative margins is an important prognostic factor [150, 151, 152].
|
|
Vena caval tumour thrombus |
Radical nephrectomy combined with vena cava thrombectomy is recommended [153]. A preoperative MRI can predict venous wall invasion [154]. Thrombectomy is associated with high mortality (5–15%) and morbidity (35–70%) which increase with the level of the thrombus [153]. An adequate technical support centre including the possibility of cardiopulmonary bypass and cardioplegia, and a trained multidisciplinary surgical team are essential for the optimal management of T3b and especially T3c tumours [155]. Survival rates at 5 years are 40–65% and 0–17% in case of metastases. Poor prognostic factors are: incomplete tumour resection, invasion of perirenal fat, lymph node metastases and invasion of the venous wall [156].
The recommendations for the treatment of locally advanced tumours are summarized in #tabr7.
|
|
Treatment of metastatic kidney cancer |
|
| IMDC classification (Heng) |
The International Metastatic RCC Database Consortium [160] (IMDC) classification is now the most widely used in clinical practice (Table 9) [161]. It was also validated in second line [162] and in non-clear cell carcinomas [163]. The medians for overall survival are 43, 23 and 8 months respectively in the good (0 factor), intermediate (1 or 2 factors) or poor (≥ 3 factors) prognosis groups [161].
|
| Treatment of metastatic kidney cancer |
|
|
The place of immediate or deferred cytoreductive nephrectomy (CN) in metastatic kidney cancer (mRCC) |
Two early prospective randomised studies (EORTC and SWOG) have shown a significant improvement in survival after cytoreductive nephrectomy (CN) prior to treatment with IFN-alpha in generally healthy patients with metastatic kidney cancer (mRCC).
In the era of anti-angiogenic treatments, a retrospective study by the International Metastatic Renal Cancer Database Consortium (IMDC) has shown a beneficial effect of CN on survival (more than 12 months survival and with less than 4 points according to the IMDC score) [167]. Two prospective randomised studies evaluated the usefulness of CN in mRCC: CARMENA and SURTIME. The CARMENA trial evaluated the benefit of CN in addition to sunitinib while the SURTIME trial evaluated the benefit of immediate CN versus deferred CN after sunitinib treatment.
The CARMENA trial reported the non-inferiority of sunitinib alone versus CN followed by sunitinib (median overall survival: 18.4 versus 13.9 months; HR: 0.89; 95%: 0.71–1, 10; non-inferiority limit: ≤ 1.25) in patients with an mRCC with intermediate or poor prognosis according to the MSKCC model [168].
The SURTIME trial showed no benefit in progression-free survival at 28 weeks (amended primary endpoint) in patients with mRCC treated with immediate versus deferred CN in combination with sunitinib (42% versus 43%, p = 0.61). On the other hand, there was a signal in favour of a prolongation of overall survival (secondary endpoint) in the delayed CN group (32.4 [95% CI: 14.5–65.3] versus 15 [CI 95%: [9.3–29.5] months; p = 0.03) However, the trial recruited only a small number of patients and lacked robustness [169].
In light of these two prospective trials, CN should not be recommended as a first-line treatment in patients with a poor prognosis. The question of deferred nephrectomy in patients with a good or intermediate prognosis, a low metastatic volume, and who are asymptomatic or have few symptoms can be discussed on a case by case basis. In this situation, a primary systemic therapy can identify patients who may benefit secondarily from CN. Pre-treatment with sunitinib is not associated with an increase in surgery-related morbidity [169]. This two-step approach was validated by the IMDC consortium based on retrospective data, which showed a median overall survival of 46, 19 and 10 months in patients treated respectively with sunitinib followed by CN, CN followed by sunitinib and sunitinib alone [170]. The post-hoc analysis in the CARMENA study identified a subgroup of patients in the intermediate-risk population who could benefit from CN: patients with a single IMDC risk factor, patients with a single metastatic (ideally pulmonary) site, and patients who responded well to primary therapy with sunitinib and underwent secondary surgery.
The levels of evidence and recommendations for CN are indicated in #tabr8.
|
|
Local treatment of metastases |
The literature on the surgical treatment of kidney cancer metastases includes only retrospective series with highly selected patients. Therefore, the recommendations are to be followed having in mind that the level of evidence is very low.
Local treatment of metastases may be justified in several situations:
• | For symptomatic treatment,
|
• | To prevent local complications,
|
• | To defer the initiation of a systemic treatment,
|
• | To achieve complete remission and consider a therapeutic break.
|
In 2014, a systematic review of kidney cancer metastasis surgery, including 16 studies with a total of 2,235 patients, concluded that complete treatment of metastases was associated with a specific survival of 41 months vs. 15 months in the absence of treatment and/or with incomplete treatment [171]. The benefit in survival provided by a complete treatment concerned all metastatic sites (lungs, liver, bone, pancreas) and in particular, reached 142 vs 27 months for liver metastases (p = 0.003).
Metastatic surgery can only be envisaged when it is estimated that it will be complete, in a patient in good general health, with a limited number of metastatic sites and a slowly progressive disease [171, 172, 173]. Complete surgical excision is the main prognostic factor of survival. In a recent series of 586 patients, survival at 2 years was 84% with complete resection vs. 54% with incomplete resection (p < 0.001) [174].
For pulmonary metastases, patients who benefit most from surgical excision are those: (1) for whom a complete treatment is feasible (2) who have less than six lung lesions and (3) for whom the time between nephrectomy and excision of the metastases is more than 36 months [175]. Multiple metastases, lymph node invasion, short time to metastasis, large metastases, and incomplete resection are all factors that contribute to a poor prognosis after surgical treatment of lung metastases [176].
In case of a single bone metastasis, surgical excision and stabilisation improves overall survival at 5 years by 24% compared to medical treatment alone [177]. Several metastatic sites and a poor prognosis group according to Heng are criteria to withhold bone metastasis surgery [178]. Metastases can be embolised to reduce bleeding prior to surgery or to reduce symptoms of bone or paravertebral metastases [179].
Brain metastases have a particularly poor prognosis. An age below 70 years and tumour size are the main risk factors for brain metastases in kidney cancer patients [180]. General health, number of brain lesions and control of the primary disease are the main prognostic factors for overall survival. Medians for overall survival ranging from 7.5 to 24 months have been reported [181, 182]. Surgery is not the first-line treatment for single brain metastases for which stereotactic radiotherapy is often chosen [183].
Stereotaxicradiotherapy has demonstrated superiority over conventional fractionated radiotherapy with a high rate of local control (> 90%) and low morbidity [184, 185, 186, 187, 188]. An equivalent biological dose of more than 100 Gy is required to achieve an ablative effect [185, 186,189]. Continuing anti-angiogenic treatment during radiotherapy does not appear to increase the toxicity or risk of complications [190, 191]. In practice, and according to expert opinion, it is recommended to stop anti-angiogenic treatments during radiotherapy of visceral metastases and to continue it during treatment of bone metastases.
For brain metastases, surgery or stereotactic radiotherapy provides similar and superior results to panencephalic radiotherapy [192]. Panencephalic radiotherapy should be reserved for patients with many lesions or those with a poor prognosis [193].
For radiotherapy of extra-cranial metastases, a single dose (≥ 24 Gy) seems to provide better local control than hypofractionated radiotherapy [194].
When radiotherapy is considered for analgesic purposes, a single dose of 8 Gy could have the same efficacy and less toxicity than a multi-fractionated dose of 20 Gy [195].
Limited data is available on the use of ablation therapies for metastases. Retrospective studies report local control rates at 3–4 years of 77% to 91% for pulmonary and adrenal sites [196, 197, 198, 199, 200]. RF may be considered in case of a single or few metastases that do not qualify for surgery in patients with a good or intermediate prognosis. For the treatment of pulmonary metastases, the main complication is pneumothorax (42% to 89%), which requires pleural drainage in 7% to 25% of the cases [197].
The levels of evidence and recommendations concerning the indications for local treatments for metastases are provided in #tabr9.
|
| Medical treatment of clear cell renal cell carcinoma |
Up until 2005, the medical treatment of metastatic kidney cancer was based on cytokines (Interferon and Interleukin-2).
Between 2005 and 2015, targeted therapies transformed therapeutic practices. These drugs can work either by direct inhibition of the Vascular Endothelial Growth Factor (VEGF) its receptor (VEGFR) or inhibition of the PI3K/AKT/mTOR pathway in the tumour cell. In 2020, seven targeted therapies are available and reimbursed in France [201, 202, 203, 204, 205, 206, 207, 208]:
• | Five tyrosine kinase inhibitors (TKIs) (sunitinib, sorafenib, pazopanib, axitinib and cabozantinib),
|
• | Two mTOR inhibitors (temsirolimus and everolimus) [ 6, 7, 8, 9, 10, 11, 12, 13], |
• | Bevacizumab (VEGF inhibitor), tivozanib and lenvatinib have European approvals but are not available in France.
|
In 2015, immunotherapy with immune checkpoint inhibitors was added to the armamentarium. The molecules that have demonstrated efficacy in kidney cancer are nivolumab (anti PD-1), ipilimumab (anti CTLA 4), pembrolizumab (anti PD-1) and avelumab (anti PD-L1).
Treatment recommendations vary according to the tumour histology and the prognostic groups [209].
The recommendations are mainly for clear cell renal cell carcinomas and depend on the prognostic classification and treatment line.
In patients with a good or intermediate prognosis, the start of treatment can often be deferred. Due to the often slow evolution of some mRCCs, an initial observation period is recommended [209].
Since 2018, several major studies have been published on the management of metastatic kidney cancer. These recent studies have changed the way patients are managed. The principal studies report on the efficacy of combinations of immunotherapy and anti-angiogenic drugs.
|
|
The Checkmate-214 (NCT02231749) trial – nivolumab plus ipilimumab versus sunitinib |
The Checkmate 214 trial is a randomised phase 3 trial that evaluated the efficacy of the ipilimumab-nivolumab combination versus sunitinib as a first-line treatment for metastatic clear cell renal cell carcinoma [210, 211]. In patients in the intermediate and poor risk groups, with a minimum follow-up of 42 months the analysis showed a superiority of the immunotherapy combination in progression-free survival (12 vs. 8.3 months, p < 0.01), objective response rate (42% vs. 26%, p < 0.0001) and overall survival (47 vs. 26.6 months, HR 0.66, p < 0.0001) [212].
There was also a complete response rate of 10% for combination immunotherapy versus 1.4% for sunitinib.
|
|
The Keynote-426 (NCT02853331) trial – pembrolizumab plus axitinib versus sunitinib |
The keynote-426 trial is a randomised phase 3 trial that evaluated the efficacy of the pembrolizumab-axitinib combination versus sunitinib as a first-line treatment for metastatic clear cell renal cell carcinoma [213]. Analysis with a minimum follow-up of 23 months reported a benefit of the combination on progression-free survival (15.4 vs. 11.1 months, p < 0.001) and the objective response rate (60.2% vs 39.9%, p < 0.001). The median overall survival was not achieved for the combination (89.9% vs 78.3%; HR: 0.68, p < 0.0001).
The complete response rate was also higher in the pembrolizumab-axitinib combination group (9% vs. 3%).
|
|
The JAVELIN-Renal (NCT02684006) trial – nivolumab plus axitinib versus sunitinib |
The JAVELIN-Renal 101 trial is a randomised phase 3 trial that evaluated the efficacy of the avelumab-axitinib combination versus sunitinib as a first-line treatment for metastatic clear cell renal cell carcinoma [214]. Progression-free survival was more significant for the avelumab-axitinib combination in both the PD-L1 positive population and the overall population (13.3 vs. 8.0 months; p < 0.001) [215]. In the overall population, the objective response and complete response rates were 52.5% and 3.8% for the combination arm versus 25.2% and 2% for the sunitinib arm, respectively.
The avelumab-axitinib combination only has preliminary data on overall survival and is not reimbursed in France at present.
|
|
The Cabosun trial (NCT01835158) – Cabozantinib versus Sunitinib |
Cabozantinib received European MA in May 2018 following the Cabosun trial [216]. This randomised phase 2 trial showed a progression-free survival benefit of cabozantinib versus sunitinib (HR 0.48 [95% CI 0.31–0.74]; p = 0.0008) as a first-line treatment in metastatic patients with an intermediate or poor prognosis. Cabozantinib did not obtain reimbursement authorisation as a first line treatment in France.
Considering these results, the following recommendations can be made:
In patients with a good prognosis, the pembrolizumabaxitinib combination is recommended with a high level of evidence. In patients with contraindications to immunotherapies, pazopanib or sunitinib are recommended.
In patients with an intermediate or poor prognosis, nivolumab-ipilimumab or pembrolizumab-axitinib combinations are recommended with the same high level of evidence. In patients with contraindications to immunotherapies, pazopanib and sunitinib are recommended.
In the event of failure of an anti-VEGFR treatment, two drugs are recommended: nivolumab [217] and cabozantinib [218]. The options are axitinib and sorafenib.
There is no randomised data to define the best therapeutic sequence after double immunotherapy. The options are based on the use of targeted anti VEGFR therapy (expert opinion).
There is no randomised data to define the best therapeutic sequence after an immunotherapy-TKI combination. Options are based on the use of targeted therapy (expert opinion).
After an anti-angiogenic sequence followed by nivolumab, cabozantinib is the drug of choice. Some options are axitinib, sorafenib and everolimus.
After an anti-angiogenic sequence followed by cabozantinib, nivolumab is the molecule of choice. Some options are axitinib, sorafenib and everolimus.
There is no randomised data to define the best therapeutic sequence after double immunotherapy or an immunotherapy-TKI combination. Options are based on the use of targeted sequential therapy (expert opinion).
Recommendations for first line and second line treatments are depicted in Table 10 and Table 11.
|
| Medical treatment of non-clear cell renal cell carcinoma |
There are no phase 3 trials for metastatic non-clear cell renal cell carcinoma.
Inclusion in a clinical trial should be encouraged whenever possible.
Based on subgroup trials or randomised phase 2 trials, sunitinib is the first option [219, 220, 221].
In case of a sarcomatoid component, analysis of the subgroup studies showed very encouraging results in favour of combination immunotherapy strategies or immunotherapy + anti-VEGFR combination strategies (ipilimumab + nivolumab, axitinib + pembrolizumab and avelumab + axitinib).
For collecting duct carcinomas (Bellini carcinomas) or medullary carcinomas, platinum doublet chemotherapy is a possible option.
Randomised trials are under way on papillary carcinomas to define the place of MET inhibitors [222].
|
|
Cystic renal cell carcinomas |
Kidney cancers have a cystic component in 5–7% of the cases. In general, cystic tumours are not aggressive, of low-grade, and the most common histological subtype is clear cell carcinoma [223, 224]. Cross-sectional imaging (CT scan or MRI) is recommended to characterize cystic renal lesions. Contrast ultrasound can be performed in case of any contraindication to CT or MRI, or as a complement to improve the characterisation of complex cystic tumours (Bosniak IIF or III) [225, 226]. Cystic tumours are classified according to Bosniak’s 5-stage classification (I, II, IIF, III, IV), based on six radiological parameters: the appearance of the wall, the content of the cyst, the presence of septa and/ or calcifications, the presence of vegetations, the enhancement of the cyst wall and/or its content after injection of contrast medium [227, 228]. An update proposal for the Bosniak classification for CT and MRI was published in 2019 but should be validated before it can be considered for use in clinical practice [229].
The risk of malignancy that Bosniak initially reported for each category was recently re-evaluated in a systematic review of the literature [230]. The risk of malignancy was 9% (5–14%) for Bosniak II, 18% (12–26%) for Bosniak IIF, 51% (42–61%) for Bosniak III and 86% (81 -89%) for Bosniak IV [230].
In 2018, a CCAFU multicentric study evaluated the malignancy rates and histological characteristics of Bosniak III and IV lesions in France among 216 cystic tumours from the national uroCCR database. Experienced pathologists conducted a central review. The malignancy rates for Bosniak III and IV cysts were 69% and 91% respectively. These were mainly low stage (86% pT1-2), low grade (68% ISUP grade 1–2) and good prognosis (recurrence 1.1%, disease-specific survival 100%) tumours [223]. In a second national multicentric study, the CCAFU reported the long-term oncological outcome of 152 Bosniak IIF (6%), III (53%) and IV (41%) cystic RCCs with a median follow-up of 61 months [224]. Tumour characteristics were similar according to the Bosniak stage: clear cell carcinoma in 56% of the cases and papillary in 23% of the cases. The Bosniak category was associated with a higher prevalence of high-grade tumours (36 vs. 12%, p < 0.01) [224]. However, the Bosniak category was not predictive of oncological outcomes, with similar favourable relapse-free survival rates for Bosniak III and IV of 92% vs. 92% at 5 years and 84% vs. 83% at 10 years (p = 0.60) [224].
The management of cystic tumours is driven by the Bosniak classification. For Bosniak I and II cysts, no treatment or monitoring is recommended. A radiological surveillance period (by cross-sectional imaging) of 5 years is recommended for IIF cysts [230]. Through this surveillance, stable IIF cysts, which are benign in more than 99% of cases, can be distinguished from IIF cysts that progress to a Bosniak ≥ III (12%) and require surgical excision due to a high risk of malignancy [230]. The indications are in #tabr10.
Identification of malignancies among Bosniak III cysts is uncertain. The new Bosniak classification, including MRI, is aimed at improving the identification of malignant tumours but has not yet been validated [229]. The value of percutaneous biopsy in cystic tumours is being evaluated and is not currently recommended [38]. Bosniak III cysts are benign in approximately 50% of the cases and cystic cancers are mainly low stage/ grade with an excellent long-term prognosis. Therefore, the CCAFU considers surveillance to be a possible alternative to surgical treatment [223, 224230, 231] which can be discussed according to the complexity of the tumour and the patient’s co-morbidities. For Bosniak IV tumours, complete surgical excision is justified by the high risk of malignancy.
Intraoperative rupture of a cystic tumour is a frequent event that always raises the question of oncological risk. A recent multicentric retrospective French study reported 50 (18.7%) cases of ruptures during surgery in a series of 268 cystic tumours. There were no cases of peritoneal carcinomatosis. Rupture of the cyst was not associated with a higher risk of recurrence and the results were similar between laparoscopic robot-assisted surgery and open surgery [232]. These results confirm that cystic tumours have a low potential for malignancy. Intraoperative rupture should be avoided as much as possible but seems to have few oncological consequences. However, the CCAFU recommends surgical excision of cystic tumours without rupturing the wall during the procedure, regardless of the approach used.
Imperative situations are those where radical nephrectomy would lead to a high risk of end-stage renal failure or permanent dialysis: a single anatomical or functional kidney, bilateral renal tumours, pre-existing renal failure.
In this context, partial nephrectomy is the reference treatment.
It is recommended that a biopsy be performed prior to any decision.
Retrospective studies suggest that PN and AT in imperative indications preserve renal function identically. On the other hand, there is a higher risk of relapse with AT [233].
A CCAFU study of 284 patients published in 2017 compared 172 PNs to 112 ATs in imperative situations [234]. Recurrence-free survival was better in the PN group despite larger and more complex tumours. However, morbidity was lower for AT: fewer transfusions, shorter hospital stays and fewer complications despite a higher level of co-morbidity.
It is unlikely that there will ever be randomised studies to compare the two techniques. In these imperative situations, PN remains the reference treatment when it is technically feasible. Given the complexity of the situation, it is advisable to refer these patients to an expert centre.
|
| Tumours in kidney transplants |
Recommendations were made by the CTAFU (French urological association) on this specific topic. Tumours on kidney transplants are rare [235]. PN is the recommended first-line treatment but it is potentially complex and associated with morbidity, and therefore requires the expertise of an expert centre [236]. Transplantectomy may be discussed when the graft function is impaired, in case of locally advanced tumour or in case of symptoms. AT is also possible for small tumours of less than 4 cm [237, 238]. The decision should be made on a case by case basis by a multidisciplinary team, and should take into account the expected difficulty of the surgery, the function of the graft and the technical environment.
Table 12Summary of recommendations for the treatment of cystic lesions.LevelCharacteristics% malignancyDiagnosisIBenign cyst with thin wallNo septa or calcificationsLiquid contentNo enhancement after injection of contrast mediumBenignNo surveillanceIIBenign cyst which may contain a thin septumHyperdense cystSmall calcifications may be present in the cyst wallNo enhancement after injection of contrast mediumBenignNo surveillanceIIFNumerous thin septaMinimal thickening of walls or septaMinimal enhancement of the wall and/or septaRegular calcification of wall and septaHyperdense totally intra-renal cyst, > 3 cm5–14%Probably benignSurveillance for 5 yearsSurgical excision in case of progressionIIIThick irregular wallThick irregular calcificationsSignificant enhancement of wall and septa42–61%1) Surgical excision2) Regular surveillanceIVCyst with intracystic vegetation, enhancingThick irregular wall, enhancing81–89%Surgical excision
| Table 12 - Summary of recommendations for the treatment of cystic lesions. |
|
| Level | Characteristics | % malignancy | Diagnosis | | I | Benign cyst with thin wall
No septa or calcifications
Liquid content
No enhancement after injection of contrast medium | Benign | No surveillance | | II | Benign cyst which may contain a thin septum
Hyperdense cyst
Small calcifications may be present in the cyst wall
No enhancement after injection of contrast medium | Benign | No surveillance | | IIF | Numerous thin septa
Minimal thickening of walls or septa
Minimal enhancement of the wall and/or septa
Regular calcification of wall and septa
Hyperdense totally intra-renal cyst, > 3 cm | 5–14% | Probably benign
Surveillance for 5 years
Surgical excision in case of progression | | III | Thick irregular wall
Thick irregular calcifications
Significant enhancement of wall and septa | 42–61% | 1) Surgical excision
2) Regular surveillance | | IV | Cyst with intracystic vegetation, enhancing
Thick irregular wall, enhancing | 81–89% | Surgical excision |
|
Tumours that occur in the framework of a hereditary syndrome (VHL, MET, FLCN, or BAP1 mutations) are difficult clinical situations due to the frequently multilocular nature of the tumours and their high risk of recurrence. They require discussion in multidisciplinary teams (urologist, oncologist, oncogeneticist, interventional radiologist). Therapeutic options include: surveillance, multiple tumour excision and AT. They are discussed on a case by case basis depending on the site, size, location, complexity of the tumour and the technical facilities available.
Historical case series propose an arbitrary threshold of 3 cm above which it is advisable to treat a tumour in the context of a hereditary syndrome. This threshold would allow maximum preservation of renal parenchyma while controlling the risk of metastasis in these tumours, which are assumed to progress slowly [239, 240]. However, a recent study of tumour growth in hereditary syndrome consisting of 292 patients and 435 tumours, suggests different growth rates depending on the type of mutation. An average tumour growth rate of 0.6 cm per year is reported for BAP1, 0.37 cm per year for VHL mutations, 0.1 cm per year for FLCN mutations and 0.15 cm per year for MET mutations. The youngest patients had faster tumour growth and tumours in the same patient progressed at the same rate. This study urges caution in case of surveillance of patients with BAP1 mutations [241].
The level of evidence and recommendations for the treatment of tumours requiring urgent attention are summarized in #tabr11.
|
| Management of sporadic angiomyolipomas (AML) |
A systematic review of all available studies on sporadic AMLs was recently conducted by the EAU Renal Cell Cancer Guidelines Panel [242].
This study selected 43 articles with a systematic analysis of the risks of bias.
The following are the main facts that emerged and guide the CCAFU’s recommendations (#tabr12):
• | The level of evidence was low: almost all studies were retrospective, with no control group and a moderate to high risk of bias.
|
• | In the active surveillance of AML series, the risk of spontaneous bleeding was low (2%).
|
• | In the active surveillance series, the growth rate of AMLs was low (the volume of 11% of the AMLs increased).
|
• | In the active surveillance series, active treatment was only chosen in 5% of the cases.
|
• | There was no clear relationship between the risk of bleeding and the size of the AML, although large AMLs seemed to be the most likely to bleed; the famous 4 cm threshold that has been recommended for deciding on an active treatment is old and should no longer be considered per se [ 243]; other factors such as age, growth rate and patient preferences should be taken into account in the decision. |
• | The two treatment options besides surveillance are surgery and selective arterial embolization. Surgery (particularly partial nephrectomy) appears to be the most effective treatment. Embolization reduces the volume of the AML but is associated with a higher recurrence rate and requires secondary treatment in 30% of the cases.
|
|
|
Kidney cancer surveillance |
|
| The value of surveillance |
There is no real consensus on the modalities of post-treatment surveillance for kidney cancer [244]. While some retrospective series suggest a potential benefit of early detection of recurrence, no study with a high level of evidence has shown that regular surveillance has any impact on survival [245, 246].
The objectives of post-treatment surveillance for kidney cancer are:
1) To detect postoperative complications.
2) To detect local or distant metastases likely to benefit from curative or systemic treatment.
3) To monitor renal function and implement adequate nephroprotective measures.
Moreover, surveillance allows us to improve our knowledge on the progression of kidney cancer, especially when the data are integrated into a high-performance database such as The French Kidney Cancer Research Network UroCCR [247, 248].
Local recurrence is rare after excision of localised tumours. Risk increases with tumour size, the presence of a positive surgical margin, multifocality and tumour grade [249]. Over 95% of recurrences take place within the first 5 years of surveillance [250] and the first three years have the highest risk [251].
Abdominal CT is more effective than ultrasound in detecting local recurrence [250, 251].
The risk of developing a tumour on the contralateral kidney is rare (estimated at 2%) [252].
The risk of metastasis after surgery was estimated to be 30–40% with a median time to metastasis of 15 months [252, 253, 254]. The 5-year disease-specific survival after treatment of localised kidney cancer was estimated according to the UISS score at 91.1%, 80.4%, 54.7% respectively for low, moderate and high risk patients [255].
The first site of metastasis is the lung. CT scan is superior to X-ray in detecting pulmonary lesions [256].
Chest x-ray and abdominal ultrasound have little value in the surveillance of patients treated for localised kidney cancer [251,257].
Several prognostic models have been developed to predict the risk of metastases occurring post-operatively with time. The UISS system is easy to use and is applicable to the three most common histological subtypes [258, 259260, 261].
There is no consensus on the optimal duration of surveillance. The majority of recurrences take place within 5 years, particularly for patients in the low-risk group. For patients in the intermediate and high-risk groups, the cumulative incidence of metastasis in 36 months remains significant beyond 5 years (approximately 20%), justifying prolonged surveillance [262]. Late-onset metastases tend to be solitary and qualify for local treatment.
Regular surveillance of renal function is advised, especially in patients with preoperative renal failure.
|
| Regimen after surgical treatment of localised or locally advanced kidney cancer |
In the absence of a validated regimen, adapting surveillance to the risk of tumour recurrence can be recommended, and this can be simply assessed by the UISS system (Table 13).
The duration of surveillance should take into account the patient’s age, co-morbidities, and life expectancy [263].
The use of ionising radiation imaging can be minimised for patients in the low-risk group.
|
| Surveillance after ablation therapy for localised kidney cancer |
Thermal ablation requires surveillance by imaging at 2 months, 6 months and 1 year and then annually for a period that is not clearly defined.
Table 14Proposal for postoperative surveillance for localised or locally advanced kidney cancer.RiskLowIntermediateHighModalitiesCT TAPAlternation with ultrasound or renal MRI possibleCT TAP or Abdominal MRI and thoracic CT scanCT TAP Or Abdominal MRI and thoracic CT scanFrequencyIn 6 monthsThen every year for 3 yearsFinal control at 5 yearsEvery six months for two yearsThen every year for 4 yearsThen every 2 years for 4 yearsEvery six months for three yearsThen every year for 3 yearsThen every 2 years for 4 yearsDuration5 years10 years10 years
| Table 14 - Proposal for postoperative surveillance for localised or locally advanced kidney cancer. |
|
| Risk | Low | Intermediate | High | | Modalities | CT TAP
Alternation with ultrasound or renal MRI possible | CT TAP or Abdominal MRI and thoracic CT scan | CT TAP Or Abdominal MRI and thoracic CT scan | | Frequency | In 6 months
Then every year for 3 years
Final control at 5 years | Every six months for two years
Then every year for 4 years
Then every 2 years for 4 years | Every six months for three years
Then every year for 3 years
Then every 2 years for 4 years | | Duration | 5 years | 10 years | 10 years |
|
The most successful imaging are MRI and CT scans [264]. When surveillance is based on MRI, identifying pulmonary metastatic lesions requires an annual lung CT scan (without injection of iodinated contrast medium). Diagnosis of early local recurrence is often difficult and requires careful comparison with pre-therapeutic imaging. Given the difficulties in guiding biopsies, it is not used to diagnose recurrence, and a new treatment may be proposed based on the presence of an oval contrast image, most often located on the periphery of the lesion in contact with the deep part or the non-tumorous renal parenchyma.
|
| Surveillance of metastatic renal tumours |
Surveillance is typically carried out by thoraco-abdomino-pelvic CT scan every 3 to 6 months. Tumour response is assessed according to RECIST or Choi criteria. Surveillance during systemic therapy depends on the drug and the administration regimen implemented.
The guiding principles for surveillance are indicated in #tabr13.
Le cancer du rein est le 6e cancer le plus fréquent. En France, il a été relevé 15 323 nouveaux cas de cancers du rein en 2018, soit une augmentation d’incidence de 1,7 % par an chez l’homme et de 1,4 % chez la femme entre 1990 et 2018. En 2018, le cancer du rein a été responsable de 5 589 décès en France, soit un taux de mortalité de respectivement 5 et 1,5 décès pour 100 000 habitants chez l’homme et chez la femme [1]. L’âge et le sexe sont deux facteurs de risque non modifiables, avec un sex-ratio de 1,5 homme pour 1 femme et un pic d’incidence entre 60 et 70 ans [1]. Il y a deux principaux facteurs de risque modifiables du cancer du rein : le tabagisme et l’obésité [1, 2]. L’hypertension artérielle a également été identifiée comme pouvant favoriser le cancer du rein et le contrôle de la tension des patients hypertendus pourrait être bénéfique [3]. L’activité physique pourrait réduire le risque de cancer du rein, notamment en réduisant l’obésité et l’hypertension artérielle [4]. Les patients qui ont une insuffisance rénale chronique ont un risque augmenté de développer un cancer du rein (jusqu’à dix fois supérieur à celui de la population générale), avec des atteintes fréquemment bilatérales et/ou multifocales [5, 6]. La recommandation de prévention du Comité de cancérologie de l’Association française d’urologie (CCAFU) est dans le #ntabr1.
|
|
Évaluation diagnostique d’une tumeur du rein |
|
| Techniques d’imagerie : technique et résultats |
Le diagnostic et la caractérisation des masses rénales reposent sur trois techniques d’imagerie complémentaires - échographie-Doppler, tomodensitométrie et imagerie par résonance magnétique (IRM) - qui peuvent être réalisées sans ou avec injection de produit de contraste.
C’est souvent l’examen qui détecte de façon fortuite une masse rénale. Elle apporte des éléments de caractérisation essentiels : masse kystique ou solide, typique ou atypique, caractère hyperéchogène franc évocateur d’angiomyolipome (AML). Avec le Doppler, elle évalue la vascularization de la masse et peut participer au bilan d’extension vasculaire (veine rénale, veine cave inférieure). Elle participe à la surveillance active (SA) permettant de mesurer la tumeur rénale. Enfin, elle permet de guider de façon très efficace une éventuelle biopsie grâce à la visualisation du trajet de l’aiguille en temps réel.
L’injection intraveineuse d’un produit de contraste (Sonovue®) améliore la caractérisation des masses solides faiblement vascularisées, des masses kystiques atypiques et d’un thrombus veineux (tumoral vs cruorique), et le guidage de la biopsie vers les territoires non nécrosés en cas de volumineuse tumeur [7, 8, 9] ; la tolérance de cet agent de contraste est excellente en pratique clinique, sans contre-indication liée à la fonction rénale [7].
En pratique, la place de l’échographie-Doppler est limitée pour l’évaluation préopératoire des tumeurs rénales.
|
|
Produits de contraste iodés (PCI) |
Les PCI sont les agents de contraste de moins bonne tolérance, avec des réactions d’hypersensibilité dont l’incidence peut atteindre 3 % parmi lesquelles 0,04 % de réactions anaphylactiques sévères, et un risque de dégradation de la fonction rénale variant de 2 à 6 % selon la voie d’administration pour les produits de contraste de basse osmolalité [10, 11, 12]. Les patients à risque de néphropathie induite sont ceux qui présentent 1) une insuffisance rénale aiguë, 2) un débit de filtration glomérulaire (DFG) inférieur à 45 ml/min/1,73 m2 pour une injection intra-artérielle sus-rénale ou hospitalisés en soins intensifs, 3) ou dont le DFG est inférieur à 30 ml/min/1,73 m2 pour une injection intra-artérielle sous-rénale ou une injection intraveineuse (le cas du scanner). Chez les patients à risque, il faut proposer soit une autre modalité d’imagerie (IRM/échographie avec injection), soit assurer une hyperhydratation tout en prenant soin d’espacer les injections de PCI d’au moins 3 jours, de limiter la dose injectée au minimum nécessaire, et de contrôler la créatininémie 48 à 72 heures après l’injection.
L’hémodialyse réalisée après une injection de produit de contraste ne réduit pas la toxicité rénale des PCI [12]. En revanche chez les patients dialysés, il est préférable de réaliser un scanner avec injection à une IRM avec injection si le bénéfice diagnostique est équivalent. Chez les patients diabétiques traités par metformine, il n’est pas nécessaire d’interrompre le traitement en raison du risque d’acidose lactique si le DFG est supérieur à 30 ml/min/1,73 m2. Quand le DFG est inférieur à 30 ml/min/1,73 m2, la metformine doit être interrompue le jour de l’injection jusqu’au contrôle de la créatininémie effectué à 48 heures, celle-ci ne pouvant être reprise qu’en cas d’absence de modification significative de la fonction rénale. Enfin, le myélome même sécrétant et à chaînes légères n’est plus une contre-indication absolue à l’injection d’un PCI selon la fonction rénale [13].
La TDM est l’examen de référence pour l’évaluation des tumeurs du rein, en l’absence de contre-indication aux PCI. La dose de PCI doit être suffisante pour permettre de détecter le rehaussement des tumeurs hypovasculaires et des masses kystiques Bosniak III et IV (0,2 ml/kg d’un produit contenant 350 mg/ml d’iode). La TDM peut comprendre les quatre phases suivantes:
• | Une acquisition sans injection, indispensable pour définir la prise de contraste (> +20 UH entre la phase tubulaire et l’acquisition sans injection) ;
|
• | Une acquisition à la phase de la néphrographie corticale, 30 à 40 secondes après injection ;
|
• | Une acquisition à la phase de la néphrographie tubulaire, 80 à 100 secondes après injection (différente de la phase portale acquise 60 secondes après injection sur laquelle la médullaire n’est pas encore rehaussée) ;
|
• | Une acquisition tardive excrétoire.
|
Selon les indications, ces phases peuvent être combinées afin de limiter l’irradiation, l’acquisition en phase excrétoire dépendant de l’indication (recherche d’un rehaussement tardif, étude des rapports de la tumeur avec les voies excrétrices) [14, 15, 16]. Pour l’imagerie rénale, il est recommandé de ne pas laisser les patients à jeun et de ne pas opacifier le tube digestif.
La TDM biénergie et spectrale est une nouvelle technologie dont les résultats pourraient être prometteurs pour l’étude de la pathologie rénale [17]. Grâce à l’introduction de nouveaux capteurs multicouches et de reconstructeurs rapides, elle pourrait permettre en pratique courante d’accéder aux images monoénergétiques et de disposer d’une cartographie d’iode. Ces examens, moins irradiants qu’auparavant, pourraient être réalisés avec un volume de PCI inférieur à 50 ml. Elle limite les artefacts liés au pseudo-rehaussement des masses rénales centrales et les artefacts métalliques et pourrait améliorer la caractérisation des tumeurs du rein, en étant, entre autres, plus sensible au rehaussement des masses peu vascularisées (carcinomes papillaires) [18, 19, 20].
La TDM est la technique de choix pour l’identification des AML car elle détecte les îlots macroscopiques de graisse (densité < -20 UH), en sachant qu’il peut exister de façon exceptionnelle une métaplasie graisseuse associée à des calcifications dans les carcinomes à cellules claires. Les AML sans graisse macroscopique peuvent présenter une hyperdensité spontanée modérée (densité > 45 UH) et un rehaussement homogène [21].
Les lésions kystiques doivent être analysées selon la classification de Bosniak qui distingue 5 catégories selon le risque de malignité. Cette classification s’applique aux masses kystiques en dehors de tout contexte infectieux ou de polykystose autosomique. Néanmoins, il existe une importante variabilité du taux de malignité liée aux critères diagnostiques, aux biais d’études, à la technique d’acquisition et à la méthode d’imagerie (TDM vs IRM vs échographie de contraste).
La TDM apporte aussi des éléments de caractérisation tumorale pour les types de carcinomes rénaux, en fonction du caractère hypervasculaire ou homogène du rehaussement. Néanmoins, ces éléments ne sont qu’indicatifs et doivent inviter à réaliser une ponction-biopsie rénale dès que la nature du résultat pourra modifier la prise en charge.
La TDM avec injection est l’examen clé du bilan préopératoire d’une tumeur du rein. Elle doit comprendre au mieux une étude avant injection et trois phases après injection, avec des reconstructions multiplanaires et en MIP. Elle permet l’évaluation précise de la tumeur (taille, localisation, rapport avec les voies excrétrices supérieures et les vaisseaux) et de la graisse périrénale. Le classement selon les scores RENAL ou PADUA peut être utile pour prédire la complexité d’une néphrectomie partielle [22]. Elle participe au bilan d’extension locorégionale (veines, ganglions, surrénales) et à distance (poumons, foie, pancréas) et doit préciser en cas de thrombose cave le niveau de la portion supérieure du thrombus par rapport au diaphragme et à l’ostium des veines sus-hépatiques. Elle recherche une tumeur synchrone du rein controlatéral.
L’IRM est devenue plus qu’une modalité substitutive de la TDM en cas de contre-indication à l’injection d’un PCI (insuffisance rénale avec DFG < 30 ml/min, antécédent de réaction anaphylactique à l’injection d’un PCI). Elle est indiquée pour la caractérisation des masses kystiques et solides atypiques demeurées indéterminées au scanner, le bilan d’extension (en particulier vasculaire), et le suivi des patients porteurs de cancer héréditaire familial. Cependant, le bilan préthérapeutique des tumeurs du rein repose encore essentiellement sur la TDM.
|
|
Produits de contraste à base de gadolinium (PCG) [11, 12] |
Ils sont très bien tolérés en pratique clinique et la fibrose néphrogénique systémique est maintenant un effet secondaire tout à fait exceptionnel, voire disparu. Elle apparaissait chez les patients insuffisants rénaux sévères (GFR < 15 ml/min/1,73 m2) ou dialysés, et son incidence était liée à la stabilité du complexe chélatant le gadolinium. Chez les patients à risque, l’injection n’est aujourd’hui pas contre-indiquée si le bénéfice clinique est supérieur au risque, ce qui est le cas du cancer du rein, mais seuls les produits de stabilité élevée doivent être utilisés (Gadobutrol, Gadoterate meglumine et Gadoteridol). Les PCG peuvent entraîner une accumulation de gadolinium dans les noyaux gris centraux mais, à ce jour, il n’existe pas de symptomatologie neurologique spécifique liée à ces dépôts. Il existe aussi des dépôts dans l’os, le foie (asymptomatiques) et la peau, responsables de plaques érythémateuses similaires à celles de la fibrose néphrogénique systémique (mais en l’absence d’insuffisance rénale).
L’étude multiparamétrique comprend des séquences en pondération T2 axiale et coronale sans et avec saturation du signal de la graisse, en pondération T1, en écho de gradient en phase et en opposition de phase (détection de la graisse intratumorale sur la séquence en opposition de phase), de diffusion à B élevé (800 à 1 000), et enfin une séquence dynamique après injection de produit de contraste avec acquisition de temps tardifs (étude du wash-out des tumeurs, prise de contraste de la fibrose centrale stellaire de l’oncocytome).
Les séquences en pondération T2 (sans ou avec saturation du signal de la graisse) permettent de distinguer les tumeurs solides des masses liquidiennes typiques (même de taille infracentimétrique) ou atypiques, et à un moindre degré les AML (même pauvres en graisse) en hyposignal T2 (suffusions hémorragiques, formations papillaires ou cellules musculaires) [23, 24]. Les carcinomes à cellules claires et les tumeurs oncocytaires présentent souvent un hypersignal [25, 26]. La séquence dynamique en pondération T1 avant et après injection de PCG permet de distinguer les tumeurs hypervasculaires et hétérogènes (correspondant aux carcinomes à cellules claires et aux AML) des tumeurs moins rehaussées homogènes (carcinomes chromophobes) ou faiblement rehaussées (carcinomes papillaires). La présence d’une chute de signal en opposition de phase et sur les séquences en saturation de graisse n’est pas spécifique d’un AML à faible contingent graisseux, car il est présent pour de nombreux carcinomes [27]. L’IRM permet aussi d’identifier les territoires microkystiques ou les remaniements nécrotico-hémorragiques. Une zone centrale stellaire hypovasculaire est compatible avec le diagnostic d’oncocytome mais peut aussi être retrouvée dans les carcinomes rénaux [28]. L’imagerie de diffusion est très sensible pour détecter de petites tumeurs infracentimétriques difficilement caractérisées par les autres séquences, et lors du bilan d’extension ou de la surveillance pour identifier des métastases ganglionnaires, surrénaliennes, pancréatiques ou hépatiques.
Si l’IRM apporte des éléments d’orientation pour identifier les différents types de tumeurs solides, elle ne permet pas de poser un diagnostic histologique avec certitude en raison de l’absence de spécificité des différents signes combinés. La biopsie reste indispensable lorsque la conduite thérapeutique ultérieure peut être modifiée par les résultats histologiques [29].
Le fluorine-18-fluorodeoxyglucose (F-FDG) TEP-scanner est utilisé pour le bilan d’extension de nombreux cancers. Il n’a pas d’intérêt pour la caractérisation des tumeurs rénales. En revanche, il pourrait être utile au moment du bilan d’extension initial ou après chirurgie pour détecter les récidives. Une méta-analyse récente a évalué sa sensibilité à 0,86 (IC 95 % : 0,88–0,93) et sa spécificité à 0,88 (IC 95 % : 0,84–0,91) dans la détection des métastases. Cependant des études prospectives supplémentaires sont nécessaires pour définir sa place et l’information supplémentaire qu’il pourrait apporter par rapport au scanner [30].
Le bilan d’extension standard repose encore aujourd’hui sur la TDM thoracique et abdominale sans et avec injection, le balayage thoraco-abdomino-pelvien devant être réalisé au temps de la néphrographie artérielle. En cas de contre-indication absolue à l’injection d’un PCI, on pourra combiner un scanner thoraco-abdominal sans injection à une IRM abdominale sans et avec injection.
|
| Classifications anatomiques |
Différentes classifications morphométriques ont été décrites avec pour objectif d’aider le clinicien dans la planification opératoire et l’information apportée au patient en vue d’une chirurgie conservatrice [31]. Les plus anciennes sont les scores RENAL [22] et PADUA [32] mais sur les 10 dernières années 16 autres classifications ont été décrites [33]. La très grande majorité des études disponibles est de nature rétrospective. Les valeurs prédictives des scores RENAL et PADUA sont supérieures lorsque ceux-ci sont utilisés en catégoriel et en particulier pour l’estimation du risque de complications périopératoires globales ou majeures et de la durée d’ischémie rénale. Leur intérêt majeur est de fournir une catégorisation objective des caractéristiques tumorales permettant une comparabilité de la littérature scientifique.
Les modalités et indications des examens d’imagerie sont résumées dans le #ntabr2.
|
| Quels examens biologiques ? |
|
|
Bilan biologique standard |
Le bilan biologique standard d’une tumeur rénale doit comprendre:
• | le dosage de la créatinine sérique ;
|
• | la numération formule sanguine.
|
En cas de cancer métastatique, il faut y ajouter:
• | le bilan hépatique ;
|
• | les phosphatases alcalines ;
|
• | la lactate déshydrogénase (LDH) ;
|
• | la calcémie avec calcul de la calcémie corrigée ;
|
• | le bilan de coagulation.
|
L’objectif de ce bilan est d’évaluer la fonction rénale, de déterminer les facteurs pronostiques (pour une tumeur métastatique) et de dépister un éventuel syndrome paranéoplasique : anémie, polyglobulie, hypercalcémie, cholestase [34, 35].
|
|
Évaluation de la fonction rénale |
La technique de référence pour estimer le débit de filtration glomérulaire est le calcul de la clairance de la créatinine selon l’équation du Chronic Kidney Disease Epidemiology Collaboration 2009 (CKD EPI). L’équation du CKD EPI est jugée plus performante que les méthodes de Cockroft/Gault et le Modification of Diet in Renal Disease (MDRD) [36]. Il existe cependant des situations pour lesquelles le calcul de la clairance de la créatininémie ne permet pas d’évaluer avec fiabilité la fonction rénale : les situations extrêmes de masse musculaire (obésité, cachexie), l’inhibition de la sécrétion du tubule rénal (trimethoprime et fenofibrate) et l’élimination extrarénale de la créatinine par le microbiote (antibiothérapie à large spectre) [36]. Il est conseillé d’évaluer la fonction rénale séparée par une scintigraphie en cas d’insuffisance rénale ou de tumeurs bilatérales [37].
|
| Que doit comporter un compte-rendu standard d’anatomopathologie ? |
Le compte-rendu d’anatomopathologie constitue un élément clé de l’évaluation pronostique et de la prise en charge du patient. La Société française de pathologie et l’Institut national du cancer (INCa) ont élaboré des comptes-rendus standardisés dont les items doivent apparaître dans chaque conclusion pour un cancer du rein (Société française de pathologie, www.sfpathol.org/ ; Institut national du cancer www.e-cancer.fr).
Une conclusion type pour un cancer du rein doit comporter un certain nombre d’items qui sont listés dans le Tableau 1 [1, 2].
|
| Principaux sous-types histologiques |
Il n’y a pas eu de changement des sous-types histologiques depuis la dernière classification OMS 2016 des tumeurs urologiques et de l’appareil génital masculin [3, 4]. Cependant, de nombreuses entités sont encore en cours de démembrement, en particulier les tumeurs rénales à cellules oncocytaires ou les carcinomes du rein à stroma léiomyomateux (Tableau 2).
Les carcinomes du rein inclassés (environ 6 % des tumeurs malignes rénales), et qui ont un risque métastatique, répondent aux définitions suivantes : 1) tumeur ne répondant pas aux critères diagnostiques des sous-types histologiques classiques des carcinomes du rein ou 2) carcinome inclassé de bas grade à cellules oncocytaires ou 3) tumeur avec une composante sarcomatoïde pure [5].
Les autres tumeurs du rein sont beaucoup plus rares et sont d’origine hématopoïétique, mésenchymateuse, métanéphrique, néphroblastique, endocrine, germinale ou métastatique.
Il est recommandé d’utiliser la classification 2017 revue en 2019 par l’American Joint Committee on Cancer (AJCC) qui est identique à la classification pTNM 2017 de l’Union for International Cancer Control (UICC) [6, 7, 8]. Par rapport à la précédente classification pTNM de 2010, l’infiltration des cavités pyélocalicielles a été ajoutée dans le stade pT3a. La classifications pTNM est décrite dans le Tableau 3.
Plusieurs entités émergentes sont encore en cours de démembrement dont les tumeurs à cellules oncocytaires. Parmi ces tumeurs, les oncocytomes et les carcinomes chromophobes à cellules oncocytaires sont bien connus des uropathologistes avec comme point commun une positivité membranaire en immunohistochimie de CD117. La cytokératine 7 (CK7) est négative ou éparse pour les oncocytomes alors qu’elle est forte et diffuse pour les carcinomes chromophobes même si elle peut être négative dans 30 % des cas [9].
Plus récemment ont été rapportées les entités émergentes suivantes [10, 11, 12]:
• | Les tumeurs oncocytaires de bas grade ou Low-grade Oncocytic Tumours (LOT) : il s’agit d’une tumeur rénale à cellules oncocytaires d’architecture souvent solide mais qui a la particularité d’être CD117 négative et CK7 très positive. Peu de cas ont été décrits mais l’évolution semble indolente.
|
• | Les tumeurs oncocytaires de haut grade ou High-grade Oncocytic Tumours (HOT) sont des tumeurs rénales également à cellules oncocytaires d’architecture souvent solide de même profil immunohistochimique que l’oncocytome avec une positivité de CD117 et une CK7 négative ou focalement positive. Cette tumeur a la particularité de présenter de nucléoles très proéminents d’où la terminologie de haut grade alors que ce sont des tumeurs a priori non agressives souvent de petite taille.
|
|
| Oncogénétique : dans quels cas ? |
Les prédispositions héréditaires aux tumeurs du rein concernent environ 5 % des cas chez l’adulte. Il existe 11 syndromes avec 17 gènes identifiés : VHL, MET, FH, SDHA, SDHB, SDHC, SDHD, PTEN, BAP1, PBRM1, TSC1, TSC2, FLCN, MITF, CDC73, CDKN2B, HNF1β. L’incidence de ces prédispositions héréditaires est plus élevée dans les cancers non à cellules claires (12 % vs 3 % pour les carcinomes à cellules claires).
Les tumeurs du rein les plus fréquemment rencontrées dans ces prédispositions sont les carcinomes à cellules claires, papillaires, chromophobes, et les angiomyolipomes.
Les syndromes héréditaires les plus fréquents sont répertoriés dans le Tableau 4.
Les critères devant amener à proposer une consultation d’oncogénétique sont listés dans le Tableau 5.
La biopsie peut être faite sous anesthésie locale, en ambulatoire, sous guidage échographique ou scannographique. Le CCAFU conseille d’utiliser une aiguille 16–18 G de type coaxiale pour prévenir le risque de dissémination tumorale, d’éviter de biopsier en zone nécrotique et d’effecteur au moins deux prélèvements.
La performance diagnostique de la biopsie est meilleure lorsque:
• | La tumeur est solide plutôt que kystique.
|
• | Une aiguille à biopsie est utilisée plutôt qu’une aspiration à l’aiguille fine [ 38]. |
La cytoponction n’est pas performante et n’est plus conseillée [38].
Les biopsies doivent être fixées dans le formaldéhyde tamponné à 4 % qui permet l’analyse histologique, la Fluorescence in Situ Hybridization (FISH) et les séquençages génétiques. Un conditionnement non fixé en vue d’une congélation est recommandé pour les tumeurs du rein de l’enfant, mais la congélation est optionnelle pour les tumeurs du rein de l’adulte.
|
| Performance diagnostique et complications |
Dans les centres expérimentés, la biopsie a une bonne performance pour établir le diagnostic de malignité, mais il y a fréquemment des cas de biopsie non contributive (absence de tissu tumoral ou matériel histologique non suffisant pour statuer).
En 2016, deux revues systématiques de la littérature ont évalué les performances de la biopsie rénale [38, 39]:
• | Pour le diagnostic de malignité, la sensibilité et la spécificité étaient > 95 %.
|
• | Pour la détermination du sous-type histologique, la concordance biopsie/pièce opératoire était de 90 %.
|
• | Le diagnostic d’oncocytome sur une biopsie est difficile : il peut être compliqué de le distinguer d’un carcinome chromophobe et 25 % des patients ont un diagnostic final de carcinome à cellules claires [ 39]. |
• | Pour la détermination du grade nucléaire, la performance de la biopsie rénale allait de 43 à 93 %. Pour les tumeurs rénales < 4 cm, la concordance du grade était de 86 % avec une classification simplifiée haut/bas grade. Dans la majorité des cas, l’erreur de grade consistait en une sous-estimation par rapport à la pièce [ 40, 41]. |
• | Les complications majeures étaient rares (2 %) [ 38]. |
• | L’ensemencement tumoral sur le trajet de la biopsie était exceptionnel [ 42]. |
• | Le taux de biopsies non contributives pouvait aller jusqu’à 20 %.
|
La pratique de la biopsie est très variable en France et il est difficile d’en cerner les indications avec certitude. Il y a de plus en plus de questionnements sur le caractère « médico-légal » de la biopsie qui pourrait éviter un certain nombre d’exérèses de tumeurs bénignes.
La position du CCAFU est de recommander la biopsie d’une tumeur du rein lorsque le diagnostic histologique est susceptible de modifier la prise en charge thérapeutique. Il est également conseillé d’informer le patient sur la possibilité de faire une biopsie, sur ses performances et ses limites. Le Tableau 6 résume les indications conseillées et déconseillées des biopsies. Les niveaux de preuve et les recommandations sont indiqués dans le #ntabr3.
|
| Place de la biopsie dans les petites tumeurs |
Pour les tumeurs < 4 cm, la contribution diagnostique de la biopsie est de 90 % [41,43]. Les sensibilité et spécificité pour le diagnostic de malignité sont > 95 %. La concordance pour le sous-type histologique est de 96 % et de 87 % pour le grade [44].
Récemment, plusieurs études ont suggéré que la biopsie pouvait modifier la prise en charge des petites masses rénales notamment en diminuant le taux d’interventions pour les tumeurs bénignes [40].
Concernant les oncocytomes, plusieurs séries ont rapporté des résultats rassurants concernant la stratégie de surveillance après confirmation biopsique [45, 46, 47, 48, 49, 50]. La croissance des oncocytomes est lente (de 0,1 à 0,5 cm/an) mais la valeur prédictive négative de la biopsie n’est pas excellente avec des corrélations histologiques entre biopsie et pièce opératoire qui oscillent entre 65 et 100%.
|
|
Traitement des petites tumeurs du rein T1a (< 4 cm) |
|
| Place de la néphrectomie partielle (NP) |
La NP est la technique chirurgicale de référence des petites masses rénales. Elle doit répondre à trois impératifs : le contrôle oncologique, la préservation de la fonction rénale et la limitation des complications périopératoires.
La NP permet un contrôle oncologique identique à la néphrectomie totale (NT) [51]. Après NP pour tumeur T1a, la survie sans récidive à 5 ans est > 95 % [51].
Une marge chirurgicale positive augmente le risque de récidive locale mais ne semble pas avoir d’impact sur la survie spécifique [52, 53, 54]. En cas de marge chirurgicale positive, il est recommandé de faire une simple surveillance par des examens d’imagerie réguliers. La totalisation immédiate par néphrectomie n’est pas nécessaire [53,55]. En cas de tumeur agressive de haut grade et/ou de marge positive importante, il peut être discuté en RCP de faire une totalisation.
Le traitement d’une récidive locale a été peu évalué. On peut faire une néphrectomie élargie, une seconde NP ou un traitement ablatif (TA) en fonction du délai d’apparition de la récidive, du type histologique et du grade [55].
|
|
Préservation de la fonction rénale |
La NP permet une préservation optimale du parenchyme rénal, ce qui limite l’altération de la fonction rénale [56]. Cette préservation fonctionnelle permet de diminuer le risque d’évènements cardiovasculaires et pourrait augmenter la survie globale par rapport à la NT [57, 58, 59, 60]. La préservation rénale est également associée à un impact psychologique positif et à une meilleure qualité de vie [61].
La durée d’ischémie. L’impact de la durée d’ischémie sur la dégradation de la fonction rénale est discuté. L’ischémie rénale pourrait avoir un effet plus délétère chez les patients atteints d’insuffisance rénale préexistante [60]. Les données de la littérature sont contradictoires mais il est conseillé de limiter la durée de clampage du pédicule rénal à moins de 25 minutes [62]. Les techniques sans clampage ou avec clampage sélectif n’ont pas fait la preuve d’une meilleure préservation rénale par rapport à un clampage total < 25 minutes [63, 64].
La préservation du volume parenchymateux. La préservation du parenchyme rénal sain apparaît être le facteur le plus important du maintien de la fonction rénale [62,65]. Les techniques d’énucléation tumorale conservant une marge minimale de tissu sain ne semblent pas accroître le taux de récidive locale mais leur apport pour préserver la fonction rénale est incertain [1066, 67].
La NP a une morbidité significative qui est d’environ 20 % dans la littérature. Les deux complications les plus redoutées sont le saignement secondaire (faux anévrysme) et la fistule urinaire. Le taux de complications graves après NP peut atteindre 11 %. Le risque de complications est influencé par de nombreux facteurs : la complexité tumorale, l’âge, les comorbidités, l’expérience du chirurgien, le volume du centre, la voie d’abord [68, 69].
|
|
Technique : voie ouverte vs laparoscopie vs laparoscopie robot-assistée |
Quelle que soit la voie d’abord (ouverte vs laparoscopie vs robot-assistance) de la NP, il n’existe pas de différence en termes de survie spécifique et de survie globale [70, 71].
Comparée à la voie ouverte, la laparoscopie diminue les pertes sanguines et la durée de séjour. À l’inverse, les durées opératoires et d’ischémie sont plus longues. Les complications postopératoires et la fonction rénale à long terme sont similaires [70, 71]. C’est une voie d’abord techniquement difficile qui tend à disparaître. Certaines équipes proposent une embolisation préopératoire des tumeurs pour faciliter le geste opératoire et diminuer les complications postopératoires, mais c’est une technique encore en développement dont la diffusion reste modeste [73].
Comparée à la voie ouverte, la laparoscopie robot-assistée a un avantage en termes de pertes sanguines, de durée de séjour, de complication et de durée d’ischémie. Le taux de marges positives et la fonction rénale résiduelle sont similaires [7174, 75].
Comparée à la voie laparoscopique, la voie robot-assistée a un avantage en termes de durée d’ischémie, de conversion par voie ouverte, de variation du débit de filtration glomérulaire et de durée de séjour [76]. Il existe également un bénéfice en termes de taux de conversion vers une NT notamment pour les tumeurs complexes et hilaires [7176, 77].
Une étude prospective faite en 2010 en France au sein d’institutions hospitalières, universitaires et libérales avait suggéré un effet centre de la NP avec une augmentation de la morbidité et du taux de marges positives dans les centres de moindre volume [78]. Une étude plus récente du CCAFU a également montré de meilleurs résultats dans les centres de haut volume concernant la NP robotique [25,79]. S’il nous apparaît délicat de faire des recommandations sur un éventuel seuil, le CCAFU encourage les équipes à s’organiser de façon à ce que l’activité de NP soit concentrée sur quelques chirurgiens experts en fonction du volume d’activité.
Les niveaux de preuve et les recommandations concernant les indications de la NP pour les tumeurs T1a sont dans le #ntabr4.
|
| Place de la néphrectomie totale (NT) |
La NT n’est pas recommandée en première intention pour les petites tumeurs du rein. Elle peut être proposée en cas de rein non fonctionnel, de suspicion de tumeur classée T3a ou de complexité importante. En cas de tumeur jugée trop complexe, il est conseillé de demander l’avis d’un centre expert avant de décider de faire une NT.
|
|
Technique : voie ouverte vs laparoscopie vs laparoscopie robot-assistée |
Les résultats oncologiques des différentes voies d’abord sont équivalents [80]. La laparoscopie est associée à une durée d’hospitalisation plus courte, à une diminution de la consommation d’antalgiques et à une diminution du saignement opératoire [81]. Les voies d’abord laparoscopiques trans- ou rétropéritonéales ont des résultats oncologiques et de qualité de vie équivalents [82]. Très peu d’études comparent la technique robot-assistée et la laparoscopie standard dont les résultats semblent équivalents [83].
|
| Place du traitement ablatif |
Les petites tumeurs rénales peuvent être traitées par traitement ablatif (TA). Il est recommandé de faire une biopsie diagnostique auparavant. Il existe différentes techniques de TA :
• | radiofréquence (RF) et micro-ondes ;
|
• | cryothérapie ;
|
• | plus récemment, électroporation irréversible ou radiothérapie stéréotaxique.
|
Les indications de TA sont résumées dans le Tableau 7.
Le TA peut être proposé comme une option aux patients dont la tumeur peut être traitée de façon complète. Les résultats techniques et fonctionnels à long terme des TA sont bons [5184, 85]. Il n’existe pas d’étude randomisée comparant TA vs NP et les études rétrospectives publiées présentent de nombreux biais. Il semble cependant que le contrôle oncologique local après TA soit inférieur à celui de la NP [5184-87]. Certaines études rétrospectives mettent en avant une meilleure préservation de la fonction rénale comparée à la NP [88, 89]. Le taux de complications globales ou majeures semble inférieur pour les TA par rapport à la NP [3992, 93].
Comment situer les TA par rapport à la NP ? Il n’y a pas d’étude randomisée comparant les deux techniques. Toutes les recommandations se basent sur des études rétrospectives. Une méta-analyse récente de 26 études et de 11 revues systématiques a été publiée par le groupe des recommandations sur le cancer du rein de l’EAU. La conclusion était que le niveau de preuve était très faible concernant les TA et qu’il était difficile dans ce contexte de faire des recommandations par rapport à la NP. Le CCAFU recommande d’informer les patients sur le fait que les TA donnent de bons résultats oncologiques même s’ils sont inférieurs à ceux de la NP mais que les données à long terme sont incertaines.
|
| Place de la surveillance active |
La surveillance active (SA) se définit comme la surveillance régulière de la taille d’une tumeur du rein par des examens d’imagerie répétés (échographie, scanner ou IRM). Un traitement peut être proposé si la tumeur augmente de volume [94].
La biopsie n’est pas obligatoire pour proposer la SA.
Les indications préférentielles sont :
• | les patients âgés ;
|
• | les patients avec des comorbidités importantes ;
|
• | les petites tumeurs du rein < 4 cm.
|
Il n’existe pas d’essai randomisé de SA chez des patients avec une petite masse rénale. En revanche, plusieurs registres prospectifs sont en cours [95, 96].
Le principal registre multicentrique du Delayed Intervention and Surveillance for Small Renal Masses (DISSRM) a étudié la faisabilité de la SA pour les tumeurs < 4 cm et a rapporté des survies globales (92 % vs 75 % ; p = 0,06) et spécifiques (99 % vs 100 % ; p = 0,3) à 5 ans similaires entre les patients traités d’emblée (par NP ou TA) et ceux initialement surveillés [97]. L’actualisation de ces données à 7 ans confirme la faisabilité de la SA avec des survies spécifiques similaires entre NP et SA [98]. Une étude prospective non contrôlée du MD Anderson rapportait cependant une diminution de la survie globale à 2 ans pour les tumeurs de plus de 3 cm surveillées (vs chirurgie), évoquant ainsi un seuil de 3 cm pour la SA [99].
En termes de qualité de vie, comparés aux patients pris en charge par une intervention immédiate (chirurgie ou traitement ablatif), les patients sous SA sont en moins bon état de santé physique (mais ce sont des patients plus âgés avec des comorbidités) et montrent plus d’anxiété [100, 101].
La surveillance est possible pour les tumeurs T1b bien qu’on ne dispose que de données très parcellaires. Elle est réservée aux patients âgés et inopérables [102].
Les niveaux de preuve et les indications de la SA et des TA pour les petites tumeurs du rein figurent dans le #ntabr5.
La Figure 1 résume les modalités de prise en charge des petites tumeurs du rein.
Figure 1.
Algorithme de décision pour la prise en charge des petites tumeurs du rein.
|
|
Traitement des tumeurs du rein localisées > 4 cm |
|
| Place de la néphrectomie partielle |
La NP a des résultats oncologiques identiques à la NT en cas de tumeur > 4 cm. Elle permet une meilleure préservation de la fonction rénale mais semble associée à une morbidité périopératoire plus élevée [103, 104, 105].
La complexité de la tumeur peut être évaluée par les scores morphométriques (RENAL score, PADUA score, C-index). Ces scores pourraient avoir un intérêt pour prédire l’altération de la fonction rénale et le pronostic en cas de tumeur > 7 cm [106, 107, 108]. Une augmentation de la taille et de la complexité tumorales est associée à une augmentation du risque de tumeur pT3a et de récidive locale [107109, 110].
La voie d’abord laparoscopique robot-assistée semble diminuer la morbidité de la NP pour les tumeurs > 4 cm. Elle est associée à moins de saignement, moins de complications, et une durée d’hospitalisation plus courte que la chirurgie ouverte [111, 112]. Elle permet d’obtenir une morbidité périopératoire comparable à celle de la NT [113].
La NP est donc à privilégier dans cette indication lorsqu’elle est techniquement possible.
|
| Place de la néphrectomie totale |
La NT est indiquée lorsque la NP n’est pas réalisable techniquement (complexité tumorale, volume tumoral trop important, expertise chirurgicale insuffisante) ou lorsque le rein n’est plus fonctionnel.
Il n’est pas nécessaire de faire une surrénalectomie sauf en cas d’envahissement de contiguïté décelé lors de l’intervention ou d’anomalie évocatrice de lésion secondaire sur l’imagerie préopératoire [114, 115].
Le curage ganglionnaire chez les patients cN0 n’est pas recommandé. Si certaines études rétrospectives ont suggéré un éventuel bénéfice en termes de survie, une étude randomisée de l’European Organisation for Research and Treatment of Cancer (EORTC) n’a pas montré de bénéfice [116, 117].
Sur le plan de la technique chirurgicale, aucune différence n’a été rapportée quant au contrôle oncologique entre la NT laparoscopique et la NT par voie ouverte. La laparoscopie permet une diminution des pertes sanguines, de la douleur postopératoire, de la durée d’hospitalisation et de la convalescence [118]. La laparoscopie avec assistance robotique a des résultats oncologiques et fonctionnels strictement comparables à la laparoscopie standard [119, 120]. Il n’a pas été mis en évidence de différence oncologique entre la voie d’abord rétropéritonéale et la voie transpéritonéale [121, 122].
|
| Place des thermoablations |
Peu d’études ont rapporté le résultat des TA pour des tumeurs de plus de 4 cm et les durées de suivi sont courtes [123, 124]. Les données sont insuffisantes pour permettre de recommander leur utilisation dans cette indication.
Les recommandations de traitement pour les tumeurs cT1b-2 N0 M0 figurent dans le #ntabr6.
|
|
Traitement d’un cancer du rein localement avancé |
|
| Définition du cancer du rein localement avancé |
Les cancers du rein localement avancés sont ceux qui ne sont ni intracapsulaires (pT1, pT2) ni métastatiques (M1).
|
| Principes de la néphrectomie élargie |
|
|
Technique : voie ouverte vs laparoscopique et laparoscopique robot-assistée |
La chirurgie, dans cette situation, est en intention curative de traiter. L’objectif principal, quelle que soit la technique, est d’obtenir des marges chirurgicales négatives [125]. La voie d’abord standard pour les tumeurs du rein localement avancées est la voie ouverte. Plusieurs séries rapportent la faisabilité de la voie d’abord laparoscopique ou laparoscopique robot-assistée qui peuvent être utilisées sous réserve que l’on puisse obtenir des marges d’exérèse saines macroscopiquement [126, 127, 128].
|
|
Intérêt et indications du curage ganglionnaire |
Un curage ganglionnaire est recommandé en cas d’adénopathies palpables ou identifiées sur l’imagerie préopératoire [129]. L’exérèse chirurgicale d’adénopathies identifiées chez un patient non métastatique pourrait avoir un intérêt pronostique mais également thérapeutique (situation oligométastatique) [130, 131].
En l’absence d’adénopathie identifiée, l’utilité oncologique ou d’évaluation du stade tumoral n’est pas démontrée avec un taux de ganglions positifs sur le curage variant de 3 à 21 %. En cas d’atteinte ganglionnaire avérée, le taux de survie après néphrectomie est de 10 à 45 % à 5 ans [134].
|
| Quelle place pour les traitements adjuvants et néo-adjuvants? |
Les patients présentant une tumeur localement avancée ont un risque important de progression métastatique. Il est admis que 30 à 40 % des patients pris en charge pour un cancer du rein non métastatique progresseront à distance de la chirurgie [135].
La plupart des études randomisées ayant étudié l’intérêt d’un traitement adjuvant par antiangiogéniques chez les patients à haut risque de récidive après néphrectomie ont rapporté des résultats négatifs (Tableau 8) [138]. Seule l’étude S-TRAC qui a évalué l’intérêt d’un traitement par sunitinib chez les patients à haut risque de récidive a mis en évidence une augmentation de la survie sans récidive mais sans augmentation de la survie globale dans le groupe traité par sunitinib [139]. Le traitement adjuvant pourrait augmenter la survie globale dans la population de patients à haut risque, mais la définition de cette population n’est pas consensuelle [140, 141]. De nombreuses études évaluant l’intérêt de l’immunothérapie en adjuvant de la chirurgie dans les cancers à haut risque de récidive après chirurgie sont en cours [142].
Une revue systématique de la littérature a montré que la radiothérapie adjuvante était associée à une diminution du risque de récidive locale, mais sans impact sur la survie globale ni spécifique [143].
Lorsque les thérapies ciblées sont utilisées en néoadjuvant, il est observé une réponse limitée au niveau de la tumeur primitive (de 9 à 28 %) et cette stratégie thérapeutique n’est aujourd’hui pas recommandée [144, 145, 146]. La place des immunothérapies en néo-adjuvant est en cours d’évaluation et elles ne doivent être utilisées que dans le cadre des essais cliniques ou discutées en RCP au cas par cas [147]. Elles doivent être envisagées avec prudence car elles pourraient être associées à une majoration des difficultés chirurgicales liées aux remaniements inflammatoires péritumoraux post-immunothérapie [148].
|
|
En cas d’envahissement des organes de voisinage |
L’envahissement des organes de voisinage est difficile à prédire [149]. De nombreux patients cT4 sont surstadifiés et peuvent bénéficier d’une résection chirurgicale. La survie à ce stade est inférieure à 10 % à 5 ans, et l’existence de marges négatives est un facteur pronostique important [150, 151, 152].
|
|
En cas de thrombus tumoral dans la veine cave |
Il est recommandé de pratiquer une néphrectomie élargie associée à une thrombectomie cave [153]. La réalisation d’une IRM préopératoire peut prédire l’invasion de la paroi veineuse [154]. La thrombectomie est associée à une mortalité (5–15 %) et une morbidité élevées (35–70 %) qui se majorent avec le niveau du thrombus [153]. Un plateau technique suffisant incluant la possibilité de circulation extracorporelle et de cardioplégie et une équipe chirurgicale entraînée pluridisciplinaire sont indispensables pour la prise en charge optimale des tumeurs T3b et surtout T3c [155]. Les taux de survie à 5 ans sont de 40 à 65 % et de 0 à 17 % en cas de métastases. Les facteurs de mauvais pronostic sont : la résection tumorale incomplète, l’envahissement de la graisse périrénale, les métastases ganglionnaires et l’envahissement de la paroi veineuse [156].
Les recommandations de traitements des tumeurs localement avancées sont résumées dans le #ntabr7.
|
|
Traitement des cancers du rein métastatiques |
|
| Classification IMDC (Heng) |
La classification de l’International Metastatic RCC Database Consortium [160] (IMDC) est désormais la plus utilisée en pratique clinique (Tableau 9) [161]. Elle a également été validée en deuxième ligne [162] et dans les carcinomes non à cellules claires [163]. Les médianes de survie globale sont respectivement de 43, 23 et 8 mois dans les groupes de pronostic bon (0 facteur), intermédiaire (1 ou 2 facteurs) ou mauvais (≥ 3 facteurs) à l’ère des thérapies ciblées [161].
|
| Traitement du cancer du rein métastatique |
|
|
Place de la néphrectomie cytoréductrice (NCR) immédiate ou différée dans le cancer du rein métastatique (CRM) |
Deux études prospectives randomisées anciennes (EORTC et SWOG) ont montré une amélioration significative de la survie après néphrectomie cytoréductrice (NCR) avant traitement par IFN-alpha chez les patients en bon état général atteints d’un cancer du rein métastatique (CRM).
À l’ère des traitements antiangiogéniques, une étude rétrospective de l’International Metastatic Renal Cancer Database Consortium (IMDC) a montré un effet bénéfique sur la survie de la NCR (plus de 12 mois de survie et ayant moins de 4 points selon le score de l’IMDC) [167]. Deux études prospectives randomisées ont évalué l’intérêt de la NCR dans le CRM : CARMENA et SURTIME. L’essai CARMENA a évalué l’intérêt de la NCR en plus du sunitinib alors que l’essai SURTIME s’est intéressé au bénéfice d’une NCR immédiate vs une NCR différée après un traitement par sunitinib.
L’essai CARMENA a rapporté une non-infériorité du sunitinib seul vs la NCR suivie du sunitinib (survie globale médiane : 18,4 mois vs 13,9 mois ; HR : 0,89 ; 95 % : 0,71–1,10 ; limite de non-infériorité : ≤ 1,25) chez des patients avec un CRM de pronostic intermédiaire ou mauvais selon le modèle du MSKCC [168].
L’essai SURTIME n’a pas montré de bénéfice sur la survie sans progression à 28 semaines (critère de jugement principal amendé) chez les patients avec un CRM traités par une NCR immédiate vs une NCR différée en association avec le sunitinib (42 % vs 43 % ; p = 0,61). En revanche, il y avait un signal en faveur d’une prolongation de la survie globale (critère de jugement secondaire) dans le groupe NCR différée (32,4 [IC 95 % : 14,5–65,3] vs 15 [IC 95 % : 9,3–29,5] mois ; p = 0,03). Cependant, l’essai n’a recruté qu’un faible nombre de patients et manque de puissance [169].
À la lumière de ces deux essais prospectifs, la NCR ne doit pas être recommandée en première intention chez les patients de mauvais pronostic. La question d’une néphrectomie différée chez les patients de bon pronostic et de pronostic intermédiaire avec un faible volume métastatique, asymptomatique ou peu symptomatique, peut se discuter au cas par cas. Dans cette situation, un traitement systémique premier peut sélectionner les patients pouvant bénéficier secondairement d’une NCR. Un traitement préalable par sunitinib n’est pas associé à une augmentation de la morbidité chirurgicale [169]. Cette approche en deux temps a été validée sur des données rétrospectives par le consortium IMDC qui a montré une survie globale médiane de 46, 19 et 10 mois chez les patients traités respectivement par sunitinib puis NCR, par NCR puis sunitinib et par sunitinib seul [170]. L’analyse post hoc de CARMENA a identifié un sous-groupe de patients au sein de la population de risque intermédiaire qui pourraient bénéficier d’une NCR : les patients avec un seul facteur de risque IMDC, les patients avec un seul site métastatique (idéalement pulmonaire) et les patients qui ont bien répondu à un traitement premier par sunitinib et qui ont été opérés secondairement.
Les niveaux de preuve et recommandations de NCR sont dans le #ntabr8.
|
|
Traitement local des métastases |
La littérature sur le traitement chirurgical des métastases du cancer du rein ne comprend que des séries rétrospectives avec des patients très sélectionnés. Les recommandations doivent donc être prises avec la réserve d’un très faible niveau de preuve.
Le traitement local des métastases peut être justifié dans plusieurs situations:
• | à visée symptomatique ;
|
• | pour prévenir l’apparition de complications locales ;
|
• | pour différer l’instauration d’un traitement systémique ;
|
• | pour obtenir une rémission complète et envisager une pause thérapeutique.
|
En 2014, une revue systématique sur la chirurgie des métastases de cancer du rein, incluant 16 études, soit un total de 2 235 patients, a conclu qu’un traitement complet des métastases était associé à une survie spécifique de 41 mois vs 15 mois en l’absence de traitement et/ou de traitement incomplet [171]. Le gain en survie apporté par un traitement complet concernait tous les sites métastatiques (poumons, foie, os, pancréas) et atteignait en particulier 142 mois vs 27 mois pour les métastases hépatiques (p = 0,003).
La chirurgie des métastases ne peut s’envisager que lorsqu’on estime qu’elle sera complète, chez un patient en bon état général, avec un nombre limité de sites métastatiques et une maladie lentement progressive [171, 172, 173]. Une exérèse chirurgicale complète est le principal facteur pronostic de survie : dans une série récente de 586 patients, la survie à 2 ans était de 84 % en cas de résection complète vs 54 % en cas de résection incomplète (p < 0,001) [174].
Pour les métastases pulmonaires, les patients bénéficiant le plus d’une exérèse chirurgicale sont ceux : 1) pour lesquels un traitement complet est envisageable, 2) qui ont moins de six lésions pulmonaires et 3) dont le délai entre la néphrectomie et l’exérèse des métastases est supérieur à 36 mois [175]. Les métastases multiples, l’envahissement ganglionnaire, un délai court avant apparition des métastases, les métastases volumineuses et la résection incomplète sont des facteurs de mauvais pronostic après traitement chirurgical des métastases pulmonaires [176].
En cas de métastase osseuse unique, la chirurgie d’exérèse et de stabilisation vertébrale améliore la survie globale à 5 ans de 24 % par rapport au traitement médical seul [177]. Plusieurs sites métastatiques et un groupe de mauvais pronostic selon Heng sont des critères en défaveur d’une chirurgie de la métastase osseuse [178]. L’embolisation des métastases peut être proposée pour réduire le saignement avant chirurgie ou réduire les symptômes de métastases osseuses ou paravertébrales [179].
Les métastases cérébrales ont un pronostic particulièrement péjoratif. L’âge inférieur à 70 ans et la taille tumorale sont les principaux facteurs de risque de métastases cérébrales chez les patients atteints d’un cancer du rein [180]. L’état général, le nombre de lésions cérébrales et le contrôle de la maladie primitive sont les principaux facteurs prédictifs de survie globale. Il a été rapporté des médianes de survie globale allant de 7,5 à 24 mois [181, 182]. La chirurgie n’est pas le traitement de première intention des métastases cérébrales uniques pour lesquelles la radiothérapie stéréotaxique est souvent préférée [183].
La radiothérapie stéréotaxique a démontré sa supériorité sur la radiothérapie à fractionnement conventionnel avec un taux élevé de contrôle local (> 90 %) et une faible morbidité [184-188]. Une dose biologique équivalente supérieure à 100 Gy est nécessaire pour obtenir un effet ablatif [185, 186189]. La poursuite du traitement antiangiogénique durant la radiothérapie ne semble pas en augmenter la toxicité ni le risque de complications [190, 191]. En pratique, et selon un avis d’experts, il est recommandé d’arrêter les traitements antiangiogéniques pendant le traitement par radiothérapie d’une métastase viscérale et de les poursuivre pendant le traitement des métastases osseuses.
Pour les métastases cérébrales, la chirurgie ou la radiothérapie stéréotaxique donnent des résultats similaires et supérieurs à la radiothérapie pan-encéphalique [192]. La radiothérapie pan-encéphalique doit être réservée aux patients avec de nombreuses lésions ou aux patients de mauvais pronostic [193].
Pour la radiothérapie des métastases extracrâniennes, une dose unique (≥ 24 Gy) semble apporter un meilleur contrôle local que la radiothérapie hypofractionnée [194].
Lorsque la radiothérapie est envisagée à but antalgique, une dose unique de 8 Gy aurait la même efficacité et moins de toxicité qu’une dose de 20 Gy multifractionnée [195].
Peu de données sont disponibles concernant l’utilisation des traitements ablatifs des métastases. Les premières études rétrospectives évoquent des taux de contrôle local à 3–4 ans de 77 à 91 % pour les sites pulmonaires et surrénaliens [196, 197, 198, 199, 200]. La RF peut être envisagée en cas de métastases uniques ou peu nombreuses, non accessibles à la chirurgie chez des patients de pronostic bon ou intermédiaire. Pour le traitement des métastases pulmonaires, la principale complication est le pneumothorax (42 à 89 %), qui nécessite un drainage pleural dans 7 à 25 % des cas [197].
Les niveaux de preuve et les recommandations sur les indications des traitements locaux des métastases sont dans le #ntabr9.
|
| Traitement médical du cancer du rein à cellules claires |
Jusqu’en 2005, le traitement médical du cancer du rein métastatique reposait sur les cytokines (interféron et interleukine-2).
De 2005 à 2015, les thérapies ciblées ont transformé les pratiques thérapeutiques. Ces molécules peuvent agir soit sur l’inhibition directe du Vascular Endothelial Growth Factor (VEGF), soit sur son récepteur (VEGFR), soit sur l’inhibition de la voie PI3K/AKT/mTOR dans la cellule tumorale. En 2020, sept thérapies ciblées sont disponibles et remboursées en France [201, 202, 203, 204, 205, 206, 207, 208]:
• | cinq inhibiteurs des tyrosines kinases (TKI) (le sunitinib, le sorafénib, le pazopanib, l’axitinib et le cabozantinib) ;
|
• | deux inhibiteurs de mTOR (le temsirolimus et l’évérolimus) [ 6, 7, 8, 9, 10, 11, 12, 13] ; |
• | le bévacizumab (inhibiteur du VEGF), le tivozanib et le lenvatinib disposent d’approbations européennes mais ne sont pas disponibles en France.
|
En 2015, l’immunothérapie par inhibiteur de check point immunitaire est venue agrandir l’arsenal thérapeutique. Les molécules ayant démontré leur efficacité dans le cancer du rein sont le nivolumab (anti-PD-1), l’ipilimumab (anti-CTLA-4), le pembrolizumab (anti-PD-1) et l’avélumab (anti-PD-L1).
Les recommandations de traitement varient en fonction de l’histologie tumorale et des groupes pronostiques [209].
Les recommandations concernent principalement les carcinomes rénaux à cellules claires et dépendent de la classification pronostique et de la ligne de traitement.
Chez les patients de pronostic bon ou intermédiaire : la mise en route du traitement peut souvent être retardée. Du fait de l’évolution souvent indolente de certains CRM, une période d’observation initiale est recommandée [209].
Depuis 2018, plusieurs études majeures concernant la prise en charge du cancer du rein métastatique ont été publiées. Ces études récentes dont les principales rapportent l’efficacité des combinaisons d’immunothérapie et d’antiangiogéniques ont modifié la prise en charge des patients.
|
|
Étude CheckMate-214 (NCT02231749), nivolumab plus ipilimumab vs sunitinib |
L’étude CheckMate-214 est une étude randomisée de phase 3 qui a évalué l’efficacité de l’association ipilimumab-nivolumab vs sunitinib en première ligne dans la prise en charge des cancers du rein à cellules claires métastatiques [210, 211]. L’analyse avec un suivi minimum de 42 mois a rapporté chez les patients des groupes à risque intermédiaire et mauvais la supériorité de l’association d’immunothérapie sur la survie sans progression (12 mois vs 8,3 mois ; p < 0,01), le taux de réponse objective (42 % vs 26 % ; p < 0,0001) et la survie globale (47 mois vs 26,6 mois ; HR = 0,66 ; p < 0.0001) [212].
Il faut noter également un taux de réponse complète de 10 % pour l’association d’immunothérapie vs 1,4 % pour le sunitinib.
|
|
Étude Keynote-426 (NCT02853331), pembrolizumab plus axitinib vs sunitinib |
L’étude keynote-426 est une étude randomisée de phase 3 qui a évalué l’efficacité de la combinaison pembrolizumab-axitinib vs sunitinib en première ligne dans la prise en charge des cancers du rein à cellules claires métastatiques [213]. L’analyse avec un suivi minimum de 23 mois a rapporté un bénéfice de la combinaison sur la survie sans progression (15,4 vs 11,1 mois ; p < 0,001) et le taux de réponse objective (60,2 % vs 39,9 % ; p < 0,001). La médiane de survie globale n’est pas atteinte pour la combinaison (89,9 % vs 78,3 % ; HR = 0,68 ; p < 0,0001).
Le taux de réponse complète était également plus important dans le groupe traité par la combinaison pembrolizumab-axitinib (9 % vs 3 %).
|
|
Étude JAVELIN Renal 101 (NCT02684006), avelumab plus axitinib vs sunitinib |
L’étude JAVELIN Renal 101 est une étude randomisée de phase 3 qui a évalué l’efficacité de la combinaison avelumab-axitinib vs sunitib en première ligne dans la prise en charge des cancers du rein à cellules claires métastatiques [214]. La survie sans progression était plus importante pour la combinaison avelumab-axitinib aussi bien dans la population PD-L1 positive que dans la population globale (13,3 vs 8,0 mois ; p < 0,001) [215]. Dans la population globale, les taux de réponse objective et de réponse complète étaient respectivement de 52,5 % et 3,8 % pour le bras combinaison vs 25,2 % et 2 % pour le bras sunitinib.
La combinaison avelumab-axitinib n’a pas encore de données matures en survie globale et n’est pas remboursée en France à ce jour.
|
|
Étude Cabosun (NCT01835158), Cabozantinib vs Sunitinib |
Le cabozantinib a eu l’AMM européenne en mai 2018 suite à l’étude Cabosun [216]. Cette étude de phase 2 randomisée a montré un bénéfice en survie sans progression du cabozantinib vs sunitinib (HR = 0,48 [IC 95 % : 0,31 -0,74] ; p = 0,0008) en première ligne chez les patients métastatiques de pronostic intermédiaire et mauvais. Le cabozantinib n’a pas obtenu de remboursement en première ligne en France.
Au vu de ces résultats, on peut faire les recommandations suivantes:
Chez les patients de bon pronostic, la combinaison pembrolizumab-axitinib est recommandée avec un niveau de preuve fort. Chez les patients qui ont une contre-indication aux immunothérapies, le pazopanib ou le sunitinib sont recommandés.
Chez les patients de pronostic intermédiaire ou mauvais, les combinaisons nivolumab-ipilimumab ou pembrolizumab-axitinib sont recommandées avec le même niveau de preuve fort. Chez les patients qui ont une contre-indication aux immunothérapies, le pazopanib et le sunitinib sont recommandés.
En cas d’échec d’un traitement anti-VEGFR, deux molécules sont recommandées : le nivolumab [217] et le cabozantinib [218]. Les options sont l’axitinib et le sorafénib.
Après une double immunothérapie, il n’existe pas de données randomisées permettant de définir la meilleure séquence thérapeutique. Les options reposent sur l’utilisation d’une thérapie ciblée anti-VEGFR (avis d’expert).
Après une combinaison immunothérapie-TKI, il n’existe pas de données randomisées permettant de définir la meilleure séquence thérapeutique. Les options reposent sur l’utilisation de thérapie ciblée (avis d’expert).
Après une séquence par antiangiogéniques suivie de nivolumab, le cabozantinib est la molécule de choix. L’axitinib, le sorafénib et l’évérolimus sont des options.
Après une séquence par antiangiogéniques suivie du cabozantinib, le nivolumab est la molécule de choix. L’axitinib, le sorafénib et l’évérolimus sont des options.
Les recommandations des traitements systémiques en 1re et 2e lignes sont rapportées dans les Tableau 10 et Tableau 11.
Après une double immunothérapie ou une combinaison immunothérapie-TKI, il n’existe pas de données randomisées permettant de définir la meilleure séquence thérapeutique. Les options reposent sur l’utilisation séquentielle d’une thérapie ciblée (avis d’expert).
|
| Traitement médical des carcinomes non à cellules claires |
Il n’y a pas d’étude de phase 3 pour les carcinomes rénaux métastatiques non à cellules claires.
L’inclusion dans un essai clinique doit être encouragée chaque fois que possible.
En se basant sur les études de sous-groupe ou sur des études de phases 2 randomisées, le sunitinib représentait la première option [219, 220, 221].
En cas de contingent sarcomatoïde, l’analyse des études de sous-groupe a montré des résultats très encourageants en faveur des stratégies d’association d’immunothérapie ou de combinaison d’immunothérapie + anti-VEGFR (ipilimumab + nivolumab, axitinib + pembrolizumab et avélumab + axitinib).
Pour les carcinomes des tubes collecteurs (carcinomes de Bellini), ou des carcinomes médullaires, la chimiothérapie par un doublet à base de sel de platine est une option possible.
Des essais randomisés sont en cours sur les carcinomes papillaires afin de définir la place des inhibiteurs de MET [222].
|
|
Tumeurs kystiques du rein |
Les cancers du rein ont un aspect kystique dans 5 à 7 % des cas. Les tumeurs kystiques sont généralement peu agressives, de bas grade, et le sous-type histologique le plus fréquent est le carcinome à cellules claires [223, 224]. Une imagerie en coupe (TDM ou IRM) est recommandée pour caractériser au mieux les lésions kystiques du rein. Une échographie de contraste peut être réalisée en cas de contre-indication au scanner ou à l’IRM, ou en complément pour mieux caractériser une tumeur kystique complexe (Bosniak IIF ou III) [225, 226]. Les tumeurs kystiques sont classées selon la classification de Bosniak en 5 stades (I, II, IIF, III, IV), en fonction de 6 paramètres radiologiques : l’aspect de la paroi, le contenu du kyste, la présence de cloisons et/ou de calcifications, la présence de végétations, le rehaussement de la paroi du kyste et/ou de son contenu après injection de produit de contraste [227, 228]. Une proposition de réactualisation de la classification de Bosniak pour le TDM et l’IRM a été publiée en 2019 mais elle doit être validée avant que l’on envisage de l’utiliser en pratique clinique [229].
Le risque de malignité que Bosniak avait rapporté initialement pour chaque catégorie a récemment été réévalué dans une revue systématique de la littérature [230]. Le risque de malignité était de 9 % (5–14 %) pour les Bosniak II, 18 % (12–26 %) pour les Bosniak IIF, 51 % (42–61 %) pour les Bosniak III et 86 % (81–89 %) pour les Bosniak IV [230].
En 2018, une étude multicentrique du CCAFU a évalué les taux de malignité et les caractéristiques histologiques des lésions Bosniak III et IV en France parmi 216 tumeurs kystiques issues de la base nationale uroCCR. Une relecture centrale par des anatomopathologistes expérimentés a été effectuée : les taux de malignité pour les kystes Bosniak III et IV étaient respectivement de 69 et 91 %. Il s’agissait principalement de tumeur de faible stade (86 % pT1–2), de faible grade (68 % grade ISUP 1–2) et de bon pronostic (récidive 1,1 %, survie spécifique 100 %) [223]. Dans une deuxième étude nationale et multicentrique, le CCAFU a rapporté le devenir oncologique à long terme de 152 CCR kystiques Bosniak IIF (6 %), III (53 %) et IV (41 %) avec un suivi médian de 61 [224]. Les caractéristiques tumorales étaient similaires selon le stade Bosniak : carcinome à cellules claires dans 56 % des cas, papillaire dans 23 % des cas. La catégorie de Bosniak était associée à une prévalence plus élevée de tumeurs de haut grade (36 % vs 12 % ; p < 0,01) [224]. Cependant la catégorie de Bosniak n’était pas prédictive du devenir oncologique avec des taux de survie sans récidive favorables et similaires pour les Bosniak III et IV de 92 % vs 92 % à 5 ans et de 84 % vs 83 % à 10 ans (p = 0,60) [224].
La prise en charge des tumeurs kystiques est déterminée par la classification de Bosniak. Pour les kystes Bosniak I et II, aucun traitement ni suivi n’est recommandé. Une période de surveillance radiologique (par imagerie en coupe) de 5 ans est recommandée pour les kystes IIF [230]. Ce suivi permet de distinguer les kystes IIF stables, qui sont bénins dans plus de 99 % des cas, des kystes IIF qui évoluent vers un stade Bosniak ≥ III (12 %) et qui nécessitent une exérèse chirurgicale en raison d’un risque de malignité élevé [230]. Les indications des traitements des tumeurs kystiques sont dans le #ntabr10.
L’identification des tumeurs malignes au sein des kystes Bosniak III est incertaine. La nouvelle classification de Bosniak incluant l’IRM a pour objectif de mieux identifier les tumeurs malignes mais elle n’a pas encore été validée [229]. L’intérêt de la biopsie percutanée dans les tumeurs kystiques est en cours d’évaluation et elle n’est pas recommandée actuellement [38]. Les kystes Bosniak III sont bénins dans environ 50 % des cas et les cancers kystiques sont majoritairement de faible stade/grade avec un excellent pronostic à long terme. Le CCAFU considère donc que la surveillance est une alternative possible au traitement chirurgical [223, 224230, 231] qui peut être discutée en fonction de la complexité tumorale et des comorbidités du patient. Pour les tumeurs Bosniak IV, l’exérèse chirurgicale complète est justifiée par le risque élevé de malignité.
Tableau 12Synthèse des recommandations pour le traitement des lésions kystiques.GradeCaractéristiques% de malignitéDiagnosticIKyste bénin avec une paroi fine Pas de cloisons ni de calcifications Contenu liquidien Pas de rehaussement après injection du produit de contrasteBéninAucune surveillanceIIKyste bénin pouvant contenir une fine cloison Kyste hyperdense Des petites calcifications peuvent être présentes dans la paroi du kyste Pas de rehaussement après injection du produit de contrasteBéninAucune surveillanceIIFCloisons nombreuses et fines Minime épaississement des parois ou des cloisons Minime rehaussement de la paroi et/ou des cloisons Calcifications régulières de la paroi et des cloisons Kyste hyperdense et entièrement intrarénal et > 3 cm5–14 %Probablement bénigne Surveillance pendant 5 ans Exérèse chirurgicale en cas d’évolution du kysteIIIParoi épaisse et irrégulière Calcifications épaisses et irrégulières Rehaussement significatif de la paroi et des cloisons42–61 %1) Exérèse chirugicale 2) Surveillance régulièreIVKyste avec végétations intrakystiques se rehaussant Paroi épaisse et irrégulière se rehaussant81–89 %Exérèse chirurgicale
| Tableau 12 - Synthèse des recommandations pour le traitement des lésions kystiques. |
|
| Grade | Caractéristiques | % de malignité | Diagnostic | | I | Kyste bénin avec une paroi fine
Pas de cloisons ni de calcifications Contenu liquidien
Pas de rehaussement après injection du produit de contraste | Bénin | Aucune surveillance | | II | Kyste bénin pouvant contenir une fine cloison Kyste hyperdense
Des petites calcifications peuvent être présentes dans la paroi du kyste
Pas de rehaussement après injection du produit de contraste | Bénin | Aucune surveillance | | IIF | Cloisons nombreuses et fines
Minime épaississement des parois ou des cloisons
Minime rehaussement de la paroi et/ou des cloisons
Calcifications régulières de la paroi et des cloisons
Kyste hyperdense et entièrement intrarénal et > 3 cm | 5–14 % | Probablement bénigne
Surveillance pendant 5 ans
Exérèse chirurgicale en cas d’évolution du kyste | | III | Paroi épaisse et irrégulière
Calcifications épaisses et irrégulières
Rehaussement significatif de la paroi et des cloisons | 42–61 % | 1) Exérèse chirugicale
2) Surveillance régulière | | IV | Kyste avec végétations intrakystiques se rehaussant
Paroi épaisse et irrégulière se rehaussant | 81–89 % | Exérèse chirurgicale |
|
La rupture peropératoire d’une tumeur kystique est un évènement fréquent qui pose toujours la question du risque oncologique. Une étude récente rétrospective multicentrique française a rapporté 50 (18,7 %) cas de ruptures sur une série de 268 tumeurs kystiques opérées. Aucun patient n’a présenté de carcinose péritonéale. La rupture du kyste n’était pas associée à un risque plus élevé de récidive et les résultats étaient similaires entre la chirurgie laparoscopique robot-assistée et la chirurgie ouverte [232]. Ces résultats confirment que les tumeurs kystiques ont un faible potentiel de malignité. La rupture peropératoire doit être évitée au maximum mais semble avoir peu de conséquences sur le plan oncologique. Le CCAFU recommande cependant de réaliser l’exérèse chirurgicale d’une tumeur kystique sans rompre sa paroi au cours de l’intervention, et ce quelle que soit la voie d’abord utilisée.
|
| Tumeurs en situation impérative |
Les situations impératives sont celles où une néphrectomie totale entraînerait un risque élevé d’insuffisance rénale terminale ou de dialyse définitive : rein anatomiquement ou fonctionnellement unique, tumeur rénale bilatérale, insuffisance rénale préexistante.
Dans ce contexte, la néphrectomie partielle est le traitement de référence.
Il est recommandé de réaliser une biopsie avant toute décision thérapeutique.
Des études rétrospectives suggèrent qu’en situation impérative, la NP et les TA préservent la fonction rénale de façon identique. En revanche, il y a un risque de récidive plus élevé avec les TA [233].
Une étude du CCAFU de 284 patients publiée en 2017 a comparé 172 NP à 112 TA en situation impérative [234]. La survie sans récidive était meilleure dans le groupe NP malgré des tumeurs de plus grande taille et plus complexes. En revanche, la morbidité était moindre pour les TA : moins de transfusions, durées d’hospitalisation plus courtes et moins de complications malgré des comorbidités plus élevées.
Il est peu probable que l’on dispose un jour d’études randomisées comparant les deux techniques. La NP reste dans ces situations impératives le traitement de référence quand elle est techniquement faisable. Compte tenu de la complexité de la situation, il est conseillé d’adresser ces patients à un centre expert.
|
| Tumeurs sur transplants rénaux |
Des recommandations ont été faites par le Comité de transplantation de l’Association française d’urologie (CTAFU) sur ce sujet précis. Les tumeurs sur transplant rénal sont rares [235]. La NP est le traitement recommandé en première intention mais elle est potentiellement complexe et morbide ce qui nécessite le recours à un centre expert [236]. Il peut être discuté de faire une transplantectomie quand la fonction du greffon est altérée, en cas de tumeur localement avancée ou en cas de symptômes. Les TA sont également possibles sur des petites tumeurs de moins de 4 cm [237, 238]. La décision doit être prise au cas par cas de façon multidisciplinaire en tenant compte de la difficulté attendue de la chirurgie, de la fonction du greffon et du plateau technique disponible.
Les tumeurs survenant dans le cadre d’un syndrome héréditaire (mutations de VHL, MET, FLCN, ou BAP1) sont des situations cliniques difficiles en raison du caractère fréquemment multiloculaire des tumeurs et de leur risque élevé de récidive. Elles nécessitent une discussion au sein d’équipes multidisciplinaires (urologue, oncologue, oncogénéticien, radiologue interventionnel). Les options thérapeutiques incluent : la surveillance, l’exérèse multiple de tumeurs et les TA. Elles se discutent au cas par cas en fonction du siège, de la taille, de la localisation, de la complexité tumorale et du plateau technique disponible.
Des séries historiques proposent un seuil arbitraire de 3 cm au-delà duquel il est conseillé de traiter une tumeur dans le cadre d’un syndrome héréditaire. Ce seuil permettrait de préserver au maximum le parenchyme rénal tout en contrôlant le risque métastatique chez ces tumeurs dont la croissance est supposée lente [239, 240]. Une étude récente de la croissance des tumeurs issues de syndrome héréditaire chez 292 patients et 435 tumeurs évoque cependant des rythmes de croissances différents en fonction du type de mutation. Il est rapporté une vitesse de croissance tumorale moyenne de 0,6 cm par an pour les mutations de BAP1, 0,37 cm par an pour les mutations de VHL, 0,1 cm par an pour les mutations de FLCN et 0,15 cm par an pour les mutations de MET. Les patients les plus jeunes avaient une croissance tumorale plus rapide et les tumeurs d’un même patient évoluaient au même rythme. Cette étude incite à la prudence dans le cas de la surveillance des patients atteints d’une mutation de BAP1 [241].
Les niveaux de preuve et recommandations pour le traitement des tumeurs en situation impérative sont résumés dans le #ntabr11.
|
| Prise en charge des angiomyolipomes sporadiques (AML) |
Une revue systématique de toutes les études disponibles sur les AML sporadiques a été faite récemment par le groupe des recommandations sur le cancer du rein de l’EAU [242].
Cette étude a retenu 43 articles avec une analyse systématique des risques de biais.
Voici les principaux éléments qui en ressortent et qui guident les recommandations du CCAFU (#ntabr12):
• | Le niveau de preuve est bas : la quasi-totalité des études sont rétrospectives, sans groupe contrôle avec un risque de biais modéré ou élevé.
|
• | Dans les séries de surveillance active des AML, le risque de saignement spontané est faible (2 %).
|
• | Dans les séries de surveillance active, le taux de croissance des AML est bas (11 % des AML augmentent de volume).
|
• | Dans les séries de surveillance active, un traitement actif n’est décidé que dans 5 % des cas.
|
• | Il n’y a pas de relation clairement établie entre le risque de saignement et la taille de l’AML même si les AML volumineux semblent être les plus à mêmes de saigner ; le fameux seuil de 4 cm qui a été recommandé pour décider d’un traitement actif est ancien et ne devrait plus être considéré de façon isolée [ 243] ; d’autres facteurs tels que l’âge, le taux de croissance et les préférences du patient doivent intervenir dans la décision. |
• | Les deux options thérapeutiques en dehors de la surveillance sont la chirurgie et l’embolisation artérielle sélective ; la chirurgie (particulièrement la néphrectomie partielle) apparaît comme le traitement le plus efficace ; l’embolisation permet de réduire le volume de l’AML mais est associée à un taux de récidive plus élevé et nécessite un traitement secondaire dans 30 % des cas.
|
|
|
Suivi des cancers du rein |
Il n’y a pas de réel consensus sur les modalités de surveillance après traitement du cancer du rein [244]. Si certaines séries rétrospectives suggèrent un potentiel bénéfice d’un dépistage précoce de la récidive, aucune étude de haut niveau de preuve n’a montré qu’un suivi régulier avait un impact sur la survie [245, 246].
Le suivi après traitement d’un cancer du rein a pour objectifs:
1) De détecter les complications postopératoires.
2) De dépister une récidive locale ou à distance susceptible de bénéficier d’un traitement curateur ou systémique.
3) De surveiller la fonction rénale et mettre en place des mesures de néphroprotection adéquates.
De plus, le suivi permet d’améliorer notre connaissance de l’évolution du cancer du rein notamment lorsque les données sont intégrées dans une base de données performante (exemple : Réseau français de recherche sur le cancer du rein UroCCR [247, 248]).
La récidive locale est rare après exérèse de tumeurs localisées. Le risque augmente avec la taille de la tumeur, la présence d’une marge d’exérèse positive, la multifocalité ou le grade tumoral [249]. Plus de 95 % des récidives surviennent dans les 5 premières années de suivi [250] et les 3 premières années sont les plus à risque [251].
La tomodensitométrie abdominale est plus performante que l’échographie pour dépister une récidive locale [250, 251].
Le risque de développement d’une tumeur sur le rein controlatéral est rare (évalué à 2 %) [252].
Le risque d’apparition de métastases après chirurgie a été évalué entre 30 et 40 % avec un délai médian de 15 mois [252, 253, 254]. La survie spécifique à 5 ans après prise en charge d’un cancer du rein localisé a été estimée selon le score UISS à 91,1, 80,4 et 54,7 % pour les patients à risque faible, modéré et élevé [255].
Le premier site de progression métastatique est pulmonaire. La tomodensitométrie est supérieure à la radiographie pour la détection des lésions pulmonaires [256].
La radiographie pulmonaire et l’échographie abdominale ont peu d’intérêt dans le suivi des patients traités pour un cancer du rein localisé [251,257].
Plusieurs modèles pronostiques ont été développés pour prédire le risque de survenue de métastases à distance de la chirurgie. Le système UISS est simple d’utilisation et est applicable aux trois sous-types histologiques les plus fréquents [258, 259, 260, 261].
Il n’y a pas de consensus sur la durée idéale du suivi. La majorité des récidives survient dans les 5 ans, en particulier pour les patients du groupe de faible risque. Pour les patients des groupes à risque intermédiaire et élevé, l’incidence cumulée d’évolution secondaire sur 36 mois reste significative au-delà de 5 ans (de l’ordre de 20 %), justifiant un suivi prolongé [262]. Les métastases d’apparition tardive sont volontiers solitaires et accessibles à un traitement local.
Il est conseillé de suivre la fonction rénale régulièrement notamment chez les patients qui avaient une insuffisance rénale préopératoire.
|
| Quel schéma peut être recommandé après traitement chirurgical d’un cancer du rein localisé ou localement avancé? |
En l’absence de schéma validé, on peut proposer d’adapter le suivi au risque de récidive tumorale qui peut être évalué simplement par le système UISS (Tableau 13).
La durée du suivi doit prendre en compte l’âge, les comorbidités, et l’espérance de vie du patient [263].
On peut limiter l’utilisation des examens d’imagerie irradiants pour les patients du groupe de faible risque et privilégier l’échographie ou l’IRM.
|
| Quel suivi après traitement ablatif d’un cancer du rein localisé ? |
Les ablations thermiques nécessitent une surveillance avec bilan d’imagerie à 2 mois, 6 mois puis à 1 an puis tous les ans pour une durée qui n’est pas clairement définie.
Tableau 14Proposition de suivi postopératoire après chirurgie du cancer du rein localisé ou localement avancé.RisqueFaibleIntermédiaireÉlevéModalitésTDM TAP Alternance possible avec échographie ou IRM rénaleTDM TAP ou IRM abdominale et TDM thoraciqueTDM TAP ou IRM abdominale et TDM thoraciqueFréquenceÀ 6 mois Puis tous les ans pendant 3 ans Ultime contrôle à 5 ansTous les 6 mois pendant 2 ans Puis tous les ans pendant 4 ans Puis tous les 2 ans pendant 4 ansTous les 6 mois pendant 3 ans Puis tous les ans pendant 3 ans Puis tous les 2 ans pendant 4 ansDurée5 ans10 ans10 ans
| Tableau 14 - Proposition de suivi postopératoire après chirurgie du cancer du rein localisé ou localement avancé. |
|
| Risque | Faible | Intermédiaire | Élevé | | Modalités | TDM TAP
Alternance possible
avec échographie ou IRM rénale | TDM TAP
ou
IRM abdominale et TDM
thoracique | TDM TAP
ou
IRM abdominale et TDM
thoracique | | Fréquence | À 6 mois
Puis tous les ans pendant 3 ans
Ultime contrôle à 5 ans | Tous les 6 mois pendant 2 ans
Puis tous les ans pendant 4 ans
Puis tous les 2 ans pendant 4 ans | Tous les 6 mois pendant 3 ans
Puis tous les ans pendant 3 ans
Puis tous les 2 ans pendant 4 ans | | Durée | 5 ans | 10 ans | 10 ans |
|
Les examens les plus performants sont l’IRM et la TDM [264]. Lorsque la surveillance repose sur l’IRM, la recherche de lésions secondaires pulmonaires nécessite un examen scannographique pulmonaire annuel (sans injection de produit de contraste iodé). Le diagnostic de récidive locale précoce est souvent difficile et nécessite une comparaison attentive à l’imagerie préthérapeutique. Compte tenu des difficultés de guidage de la biopsie, le diagnostic de récidive ne repose pas sur celle-ci, et un nouveau traitement peut être proposé sur la présence d’une prise de contraste ovalaire, le plus souvent située en périphérie de la lésion au contact de la partie profonde ou du parenchyme rénal non tumoral.
|
| Quel suivi en cas de tumeur du rein métastatique ? |
Le suivi est classiquement effectué par tomodensitométrie thoraco-abdomino-pelvienne tous les 3 à 6 mois. L’évaluation de la réponse tumorale est évaluée selon les critères RECIST ou de Choi. Le suivi au cours d’une thérapie systémique dépend de la molécule et du schéma d’administration utilisés.
Les principes qui doivent guider le suivi sont résumés dans le #ntabr13.
|
|
Déclaration de liens d’intérêts |
Laurence Albiges : Consultante : BMS, MSD, Novartis, Amgen, IPSEN, Roche, Pfizer, Merck, AstraZeneca, Exelixis, Peloton Therapeutics, Corvus Pharmaceuticals. Invitation congrès : MSD, BMS. Financement recherche : BMS.
Karim Bensalah : Consultant : Intuitive Surgical, MSD, IPSEN, Pfizer. Investigateur : Roche, MSD. Invitation congrès : BMS, Pfizer, IPSEN, Astellas. Financement recherche : Pfizer.
Jean-Christophe Bernhard : Consultant : Intuitive Surgical, Pfizer, Ipsen, Novartis. Investigateur : Intuitive Surgical. Invitation congrès : Pfizer, IPSEN, MSD, Pierre Fabre, Novartis.
Pierre Bigot : Consultant : BMS, Ipsen, KPL, MSD. Investigateur : BMS, IPSEN, Novartis, AstraZeneca, Pfizer. Invitation congrès : Ipsen, Novartis, Takeda, Pierre Fabre. Romain Boissier : Consultant : IPSEN, BMS, Janssen.
Jean-Michel Corréas : Consultant : Canon MS, Hitachi MS, Philipps MS, Siemens Healthineers, SuperSonic Imagine, Bracco SA, Guerbet SA, Novartis, Johnson & Johnson. Investigateur : Bracco SA, Guerbet SA.
Pierre Gimmel : Consultant : Pfizer, IPSEN, BMS. Invitation congrès : IPSEN, Pfizer, BMS.
Jean-François Hetet : Pas de conflit.
Nathalie Rioux Leclerq : Consultant : AstraZeneca, IPSEN, Pfizer, BMS.
Jean-Alexandre Long : Pas de conflit.
Arnaud Méjean : Consultant : Pfizer, IPSEN, Astellas, Ferring, Janssen, Novartis, GSK, BMS, Roche, Pierre Fabre.
François-Xavier Nouhaud : Consultant : Janssen, IPSEN, BMS, Astellas, MSD Invitation congrès : Astellas, IPSEN, Janssen. Bourse : Astellas, IPSEN.
Idir Ouzaid : Consultant : Janssen, BMS, Pfizer, MSD. Invitation congrès : Astellas, IPSEN, Janssen, BMS.