Patient-reported long-term sexual outcomes following plication surgery for penile curvature: A retrospective 58-patient study Évaluation fonctionnelle à distance d’une intervention chirurgicale pour courbure de verge : étude rétrospective d’une cohorte de 58 patients | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Penile curvature, mainly due to Peyronie's disease, may result in not only painful erections and difficulties with intromission but also a disturbed self-image, loss of penile length and possibly erectile dysfunction (ED) [11], which could also be noted for congenital curvature. The current incidence of Peyronie's disease ranges from 0.4 to 5% and the mean age of men with the disease is 53 years [22, 33, 44]. Collagenase Clostridium histolyticum injections are currently being evaluated and other medications have only shown moderate efficacy, leaving surgery as the only effective means of treating penile curvatures that are bothersome or that prevent sexual relations. The Nesbit, Yachia and diamond-shaped techniques (grouped under the term “plication surgery” here) have been described since the 1990s. These involve an intervention on the tunica albuginea opposite the plaque; they shorten the convex aspect of the penile curvature and thus usually the penis itself. Appraisals of the perceived or real shortening of the penis and the sexual satisfaction of the patient after surgery vary in the literature. The objective of the present work was to assess the sexual outcomes of patients after plication surgery to correct penile curvature, whether congenital or in the setting of Peyronie's disease, as reported by the patients themselves using a specifically developed questionnaire.
The patient population was retrieved from the database of a hospital specialized in penile surgery. The evaluation period was from January 2008 to February 2013. We thus performed a retrospective, monocentric descriptive study. All patients who underwent surgery for congenital curvature or Peyronie's disease during the evaluation period were retrieved. The employed surgical technique for any one patient was chosen in accordance with European and American guidelines as a function of curvature degree, penis size, any ED, photography or erection test during the visit and the patient's priorities [55, 66]. The proposed interventions at the hospital included: plication surgery, via Nesbit, Yachia or diamond-shaped techniques; grafting surgery, i.e., the lengthening of the concave penile aspect via the incision of the tunica at the plaque site and the placement of a graft using porcine intestinal submucosa; and approaches combining a prosthesis and curvature correction (modeling). For the present study, only patients with Peyronie's disease stable for at least six months or with congenital curvature and who had undergone plication surgery alone were included. Thus, patients who underwent grafting surgery or prosthesis placement were excluded. A single surgeon had performed all the interventions for the included patients. Indications for surgery were significant discomfort/pain/nuisance or the inability to have sexual intercourse. The degree of preoperative curvature was measured in the operating room during the initial erection test. All interventions were successful with only minimal residual curvature at the end of the intervention, as assessed with a new erection test.
At a mean of 34 months after their surgeries (range 6 to 62 months), we sent two questionnaires by mail to all of the patients: the simplified International Index of Erectile Function (IIEF5) and another postoperative self-reported questionnaire developed in-house to evaluate penile curvature corrective surgery and the effects of the surgery as perceived by the patient. This second questionnaire comprised 19 items exploring five postoperative domains: deformation, pain, sensation, erection, sexual relations. Each item had five or six possible responses (Appendix A).
During the evaluation period, there were 72 surgical interventions for Peyronie's disease or the correction of congenital curvature. Fourteen of these cases involved grafting surgery or prostheses and were thus excluded from the study. Therefore, there were 58 cases of plication surgery (i.e., those employing the Nesbit, Yachia or diamond-shaped techniques) included in the study (Figure 1). The employed technique was decided upon by the surgeon preoperatively and adjusted intraoperatively after the erection test.
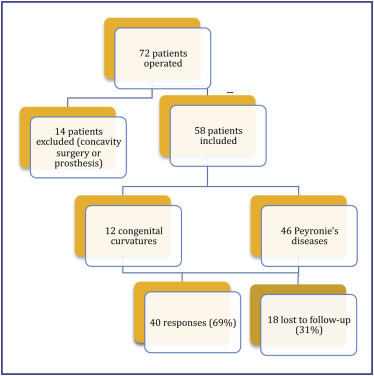 Figure 1. Flowchart.
Twelve patients (21%) with a mean age of 25 years (19–36) were operated for congenital curvature and 46 patients (79%) with a mean age of 58 years (31–83) for Peyronie's disease. Twenty-four patients (41.3%) had a preoperative curvature>60°. Forty patients responded to the questionnaires, i.e., a response rate of 69%. Seven patients (17.5%) were not having sexual relations and thus could not respond to some of the questions in the IIEF5 or in our questionnaire.
Then mean curvature measured postoperatively was 13.1° (0–60°). For 26 of them (65%) residual curvature was absent or minimal (<10°) and for three (7.9%) it was greater than 50°. None has expressed the wish to be operated again. Twenty-nine (72.5%) of the 40 respondents described a “clear” or greater loss of penile length due to the operation (Figure 2). The mean loss of length was about 2.4 centimeters (0,3cm in the congenital curvature group).
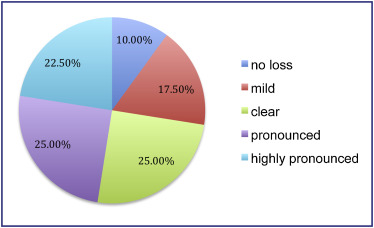 Figure 2. Postoperative functional results (Q3: Have you noticed a loss of length for your penis since the operation?). The shortened postoperative penis was considered to be at least regularly bothersome for the patient's sexuality by 19 (47.5%) patients (Figure 3).
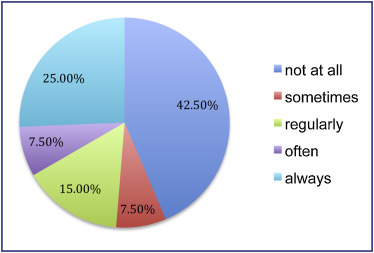 Figure 3. Postoperative functional results (Q5: Does the shorter penis bother you in your sexuality?).
The ability to achieve an erection at least sometimes was reported by 95% of the sexually active respondents. The mean postoperative IIEF5 score was 19.3/25 (23/25 in the congenital curvature group). As determined by the IIEF5, erectile function was normal (score from 22 to 25) in 32.5% of the cases. There was mild ED (score 17–21) in 30% of the cases, mild to moderate ED (score 11–16) in 15%, and severe ED (score 6–10) in 5%.
Fourteen (35%) patients reported that involuntary exit from the vagina during sexual intercourse occurred in at least one out of two sexual intercourse episodes (Figure 4).
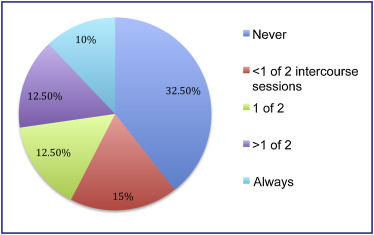 Figure 4. Postoperative functional results (Q16: How often do you experience involuntary exits from the vagina during sexual intercourse?). Sexual life after the surgery was judged as good as or better than before the surgery by 37.5% of the patients (100% in the congenital curvature group).
Twenty-three responders (57.5%) were at least satisfied with the intervention, 10 (25%) were at least unsatisfied, and seven (17.5%) had no opinion (100% satisfied in the congenital curvature group). The correlation coefficient between the degree of satisfaction with the surgery and the initial curvature was weak (r : 0.2). Thus, in our study the initial curvature appeared to play no real role in postoperative satisfaction.
Our cohort shed light on numerous aspects of the sexuality of patients with penile curvature, either congenital or due to Peyronie's disease. Plication surgery can correct the excessive curvature in the vast majority of cases (13.1° of residual curvature in our cohort) but at the price of a shortened penis. Indeed 72.5% of our patients self-reported at least a “clear” loss of penile length. This loss of length was considered bothersome for the sexuality of 47.5% of our patients and involuntary vaginal exit was reported by 35% of them.
In their guidelines, the American Urological Association (AUA) recommends surgery for the correction of penile curvature in the setting of Peyronie's disease when the curvature prevents the pursuit of a normal sexual life. No randomized studies have been done to compare plication and grafting surgery, but certain studies do give preference to plication surgery when penis size is normal, penile curvature is <60° and ED is absent. In contrast, grafting surgery or penile prostheses are recommended in the presence of a small penis, curvature >60° and/or ED [66]. The AUA guideline algorithm (Figure 5) is only moderately useful however, as it does not cover the full range of situations that may be encountered in clinical practice, for example a long penis with >60° curvature.
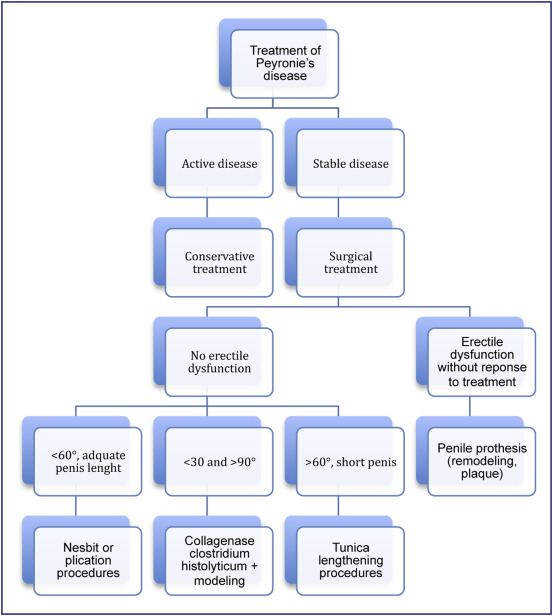 Figure 5. AUA guidelines for penile curvature. In our study, 41% of the patients (24 of 58) had a >60° penile curvature at the time of surgery, and the mean preoperative curvature was 74.2°. These numbers fall at or beyond the limits for plication surgeries as recommended by the AUA. In our center, we carefully explain the advantages and disadvantages of the various techniques to the patients and let them make the final decision. The patients who opted for plication surgery and who were included in our study had an acceptable mean residual curvature of 13.1°.
In the literature, the loss of penis length as a result of plication surgery varies widely, from 5 to 80%. Savoca et al. reported loss of penis length for 17.4% of their patients who underwent a Nesbit procedure with penetration difficulties in 2.5% of the cases [77]. Their patients had mean initial penile curvatures of 65° (30–110°), and the authors considered that the loss of penis length was significant when ≥1.5cm. However, defining loss of length in that way does not allow for an assessment of the patient's subjective impressions after the surgery, an aspect influenced greatly by the size of the patient's penis before the surgery. Recently, Kueronya and al. described patient-reported outcome data after surgery of Peyronie's disease, by plication surgery or grafting surgery [88]. As this present study, they showed that penile length loss was the most bothersome symptom after surgery in those patients. Around 78% of patients treated by plication surgery reported a subjective loss of penile length with 86% being bothered by that, more than our study explained by the fact that their questionnaire had to be answered by “yes” or “no”. Nevertheless, it showed that penile length loss is badly estimated after penile curvature surgery and surgeons misinform patients.
The self-administered IIEF5 questionnaire is validated in the setting of ED screening [99]. The mean postoperative IIEF5 score was 19.3/25 in our study, corresponding to mild ED. Versions of the International Index of Erectile Function are frequently used to assess the efficacy of penile curvature correction surgery. For example, Zucchi et al. observed a significant postoperative improvement in IIEF5 scores (from 15 to 23 of 25 possible points) in patients who underwent corporoplasty with buccal mucosa grafting [1010], and Iacono et al. reported significant postoperative improvement using the IIEF15 (from 25 to 38 of 75 possible points, P <0.01) in patients who underwent plication surgery for Peyronie's disease [1111]. Administered preoperatively, the IIEF5 is difficult to interpret because questions 3 to 5 are heavily influenced by the penile curvature, which, when significant, can make sexual intercourse impossible, thus biasing the responses to those questions. Indeed, the IIEF5 explores only the possibility of penetration and not the quality of the erection or of the sexual intercourse. In a study assessing the IIEF5 and the Lue score, Muyshondt et al. determined that only the first two questions of the IIEF5 were of use for evaluating Peyronie's disease severity preoperatively [1212, 1313], illustrating the non-pertinence of the IIEF5 in this setting. In our study, we had a very low rate of patients reporting insufficient or impossible erections (5%). Nonetheless, despite scoring well on the IIEF5, a patient could be unsatisfied with his sexual life because of functional difficulties caused by the curvature, pain encountered by his partner, loss of length following the operation or undesired exit from the vagina for example. Thus, the IIEF5 does not really lend itself to evaluating sexual satisfaction. Some teams, Levine and Natali for example, use the modified Erectile Dysfunction Index of Treatment Satisfaction (EDITS) questionnaire, validated in 1999. The advantages of the modified EDITS are that it can be adapted to any treatment of ED, medical or surgical, and that it has a sub-section for the sexual partner. Its disadvantages are that it has not been validated for Peyronie's disease and it does not evaluate rigidity or the quality of sexual intercourse [1414]. There are other questionnaires currently available. The Peyronie's Disease Index (PDI) was first described in 2002 by Shabsigh then in 2003 by Levine. It comprises 35 questions covering penile curvature as well as the notions of sexual activity, desire and satisfaction. However, the PDI has not been validated in a large-scale study as of this writing. Its questions are largely oriented toward the history of the Peyronie's disease and the quality of erections [1515]. The Lue score [1313] is useful for orienting surgery and calculating Peyronie's disease severity but not for evaluating postoperative follow-up or the patient's impressions. It evaluates pain, curvature degree and plaque size, each on a 5 point scale. It has the advantage of providing objective and precise responses for these domains and thus good reproducibility. It is often used in studies for the preoperative evaluation of patients. The Peyronie's disease questionnaire (PDQ) was recently validated in patients receiving collagenase treatment for Peyronie's disease [1616]. The PDQ explores problems and pain in sexuality caused by the Peyronie's disease and how bothersome certain aspects may be. It necessitates an evaluation both before and after plication surgery. Finally, the Self-Esteem and Relationship (SEAR) questionnaire explores four domains of self-esteem. Tal et al. showed that there was significant improvement in three of the four SEAR domains following plication surgery for Peyronie's disease, whereas the was little change in IIEF5 results [1717].
In our study, 37.5% of the patients reported a sexual life after the surgery as good as or better than before and 75% reported that they were at least not unsatisfied with the surgery. This suggests that patient satisfaction with the surgery seems to be not necessarily correlated with an improvement in sexual life or with the initial penile curvature. To our knowledge, our study is the first to illustrate this. These results may be explained in several ways. First, the criteria used to judge surgical efficacy are residual deformation and IIEF5 results. The IIEF5 reflects the postoperative sexual activity of patients badly, as demonstrated in our study, where the mean residual curvature was 13.1° and the mean IIEF5 score was 19.3/25, “successful” results coherent with those in the literature [1010, 1111]. However, these criteria cannot give a complete picture of postoperative patient sexuality in that they do not evaluate the feasibility of sexual intercourse. The questionnaire that we developed has the advantage of focusing specifically on the postoperative results of plication surgery for penile curvature and analyzing their consequences on erection quality, sexual relations quality, and patient perceptions as concerns the results of the surgery. Our results underline the need for a “reality check” when providing patients with preoperative information. Peyronie's disease progresses over months and significantly alters the sexual life of the patient and his self-image. Our high dissatisfaction rate (25%) may find its roots in the patient's hope of recovering his former sexual life completely. The results of our questionnaire illustrate how important it is to provide patients with clear and honest information as to what the surgery can and cannot do. It must be made clear to patients that a complete recovery of their former sexual life will not happen, that the penis will be shorter due in part to the remaining plaque, and that they may encounter problems during intercourse, including involuntary exits from the vagina. Nevertheless, the present study had some limits such as the retrospective nature of the study or the relatively small population sample even if this was one of the biggest in the literature only on plication surgery. The amount of non-responders (31%), of patients who didn’t have any sexual activities, and the lack of a preoperative questionnaire were also limits of our study. Finally, it does not consider patient psychological aspects. Depression, sometimes necessitating treatment, can occur in patients with Peyronie's disease. For example, Smith et al . illustrated a high prevalence of emotional (81%) and relationship (54%) difficulties in a population of 254 patients with Peyronie's disease. They reported that loss of penis length and the inability to have sexual intercourse were highly predictive (P <0.05) of these psychological difficulties [1818].
In the present study, patients who underwent plication surgery to correct penile curvature had good objective results for residual curvature and erectile function. However, the rate of dissatisfaction for these patients was high (25%) and that of maintained or improved quality of sexual life rather low (35%), possibly due to loss of penile length and resulting involuntary exits from the vagina. New pre- and postoperative questionnaires integrating psychological and sexual relations aspects need to be developed, assessed and validated to provide pertinent evaluation tools in this surgical setting. Preoperative penile length must be carefully measured and carefully considered when deciding upon a surgical technique. Surgery should be avoided if sexual intercourse is still possible. When it is needed, the patient must be clearly informed on the probable loss of penis length and the risk of involuntary exits from the vagina. The psychological impact of penile curvature and its correction should not be neglected.
The authors declare that they have no competing interest.
Supported by a grant from the Bibliothèque scientifique de l’Internat de Lyon and les Hospices Civils de Lyon. Appendix A. Supplementary data
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
© 2016
Elsevier Masson SAS. Tous droits réservés. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



